The modern institutional healthcare landscape is an intricate, rapidly evolving ecosystem. Within this dynamic environment, the roles and responsibilities of a hospital pharmacist have expanded far beyond the traditional, historical duties of compounding and dispensing medications. Today, hospital pharmacy practice has evolved into a highly clinical, patient-centered specialty that serves as a cornerstone of modern inpatient pharmacy services.

Historically, the hospital pharmacist role was viewed primarily through an operational lens—ensuring that the right drug reached the correct nursing unit. However, contemporary healthcare demands a more sophisticated approach to medication management in hospitals. With the increasing complexity of pharmacotherapy, the rise of highly specialized biologic agents, and the ever-present challenge of preventing multi-drug interactions, the clinical pharmacist responsibilities have shifted to the frontlines of direct patient care.
The modern hospital pharmacy department acts as the therapeutic nerve center of the institution. By bridging the gap between clinical diagnosis and safe drug administration, hospital pharmacists directly impact patient clinical outcomes, reduce the length of hospital stays, and safeguard institutional resource utilization. Whether analyzing serum drug concentrations in the intensive care unit or redesigning the institutional drug distribution system, these professionals ensure that patient safety remains paramount.
Understanding Hospital Pharmacy Practice
What Is Hospital Pharmacy?
Hospital pharmacy practice refers to the specialized discipline of pharmacy practice that takes place within institutional healthcare settings, including general hospitals, specialized clinics, rehabilitation facilities, and long-term care centers. Unlike other sectors of the profession, the hospital pharmacy department operates in direct alignment with the institution’s overarching clinical and operational goals.
Objectives of Hospital Pharmacy Services
The primary objective of hospital pharmacy services is to ensure the safe, effective, appropriate, and cost-effective use of medications throughout the entire facility. This is achieved by:
- Minimizing medication errors through robust multi-layer verification systems.
- Optimizing therapeutic outcomes via direct participation in clinical pharmacy services.
- Maintaining strict inventory control and financial sustainability within the hospital pharmacy management framework.
- Fostering a culture of continuous quality improvement through medication safety initiatives.
How Hospital Pharmacy Differs from Retail Pharmacy
While both sectors require profound pharmacological expertise, their operational environments and clinical depths differ substantially:
| Feature | Hospital Pharmacy Practice | Retail/Community Pharmacy |
| Primary Focus | Acute and complex clinical care, multi-disease management, and multidisciplinary collaboration. | Ambulatory care, wellness, direct retail dispensing, and community accessibility. |
| Patient Interaction | Focused on inpatient medication chart review, ward rounds, bedside discharge counseling, and high-risk interventions. | Focused on outpatient prescription filling, retail point-of-sale counseling, and preventative health services. |
| Formulary Control | High. Restructured strictly by an institutional Pharmacy and Therapeutics (P&T) Committee. | Low to Moderate. Governed broadly by open commercial drug markets and insurance formularies. |
| Interprofessional Contact | Continuous, face-to-face integration with physicians, nurses, and specialized healthcare teams. | Mostly episodic communication via telephone or electronic prescribing portals for clarifications. |
Importance of Hospital Pharmacists in Modern Healthcare
As medical science advances, the prevalence of polypharmacy—especially among aging populations with complex comorbidities—has skyrocketed. Hospital pharmacists provide a crucial layer of defense against therapeutic duplications, inappropriate dosing, and adverse drug events. According to data from the American Society of Health-System Pharmacists (ASHP), institutional settings that integrate pharmacists directly into care teams experience a significant drop in preventable drug errors, highlighting the essential nature of the functions of hospital pharmacist teams in contemporary medicine.
Roles and Responsibilities of a Hospital Pharmacist in Patient Care
At its core, the clinical involvement of a hospital pharmacist centers on executing comprehensive medication management in hospitals. Every medication order entered into a hospital’s electronic system must undergo rigorous evaluation before administration.
Prescription Verification and Clinical Review
Prescription verification is not a mechanical checklist; it is a sophisticated cognitive process. The pharmacist reviews the medication order against the patient’s complete electronic health record (EHR). This involves cross-checking:
- Patient-Specific Metrics: Age, weight, body surface area, and renal function (calculated via creatinine clearance).
- Pathophysiological Contraindications: Evaluating if a drug could exacerbate an existing comorbid condition (e.g., avoiding non-selective beta-blockers in severe asthmatic patients).
- Dosing Optimizations: Ensuring that narrow therapeutic index medications are dosed accurately to prevent systemic toxicity.
Medication Therapy Management (MTM) and Monitoring
Once a drug is verified and administered, the hospital pharmacist’s responsibility transitions into continuous monitoring. Through systematic clinical reviews, pharmacists track subjective and objective patient data to measure therapeutic response. For instance, if a patient is prescribed an anticoagulant, the pharmacist continuously monitors coagulation panels (such as INR or aPTT) alongside clinical signs of bleeding or thrombosis to dynamically adjust dosages.
Preventing Medication Errors and Assessing Interactions
Inpatient pharmacy services act as the ultimate barrier against catastrophic drug combinations. Pharmacists use advanced clinical screening methods to intercept major drug-drug, drug-food, and drug-laboratory interactions.
Practical Hospital Example: A patient on a stable maintenance dose of a calcineurin inhibitor (e.g., tacrolimus) following an organ transplant is prescribed an azole antifungal (e.g., voriconazole) for a suspected systemic infection. A clinical pharmacist immediately recognizes that voriconazole is a potent CYP3A4 inhibitor, which will cause tacrolimus levels to spike to toxic, nephrotoxic ranges. The pharmacist proactively intervenes, calculating an empirical dose reduction for tacrolimus and scheduling immediate trough level monitoring.
Adverse Drug Reaction (ADR) Monitoring
When an unexpected or noxious response to a medication occurs within the hospital, the pharmacist coordinates the tracking, management, and subsequent reporting of the event. This feed directly populates internal safety registries and national Pharmacovigilance networks, contributing to the global body of knowledge regarding drug safety.
Roles and Responsibilities of a Hospital Pharmacist in Medication Safety
Medication safety is an independent, highly specialized domain within institutional practice. A dedicated medication safety pharmacist focuses exclusively on structural system designs to eliminate opportunities for human error.

High-Alert Medication Management
High-alert medications are drugs that bear a heightened risk of causing significant patient harm when used erroneously. Examples include intravenous anticoagulants, insulins, chemotherapeutic agents, and concentrated electrolytes (like potassium chloride). Hospital pharmacists institute strict guardrails for these substances, such as:
- Enforcing independent dual-verification workflows prior to dispensing.
- Utilizing specialized auxiliary labeling (e.g., high-visibility warning stickers).
- Configuring specific “hard stops” within the hospital’s smart infusion pumps.
Look-Alike Sound-Alike (LASA) Medication Control
Misidentifying medications due to visual packaging similarities or orthographic/phonetic resemblances is a frequent source of error. Pharmacists mitigate this risk by applying Tall Man Lettering techniques (e.g., separating hydrOXYzine from hydrALAzine) on electronic screens and storage bins, and physically segregating these products within the central pharmacy vaults.
Pharmacovigilance and Incident Reporting
When a near-miss or a medication error does reach a patient, the hospital pharmacist spearheads a Root Cause Analysis (RCA). Rather than focusing on individual blame, the pharmacist evaluates systemic flaws—such as ambiguous ordering screens, workflow interruptions, or lighting inadequacies—and introduces corrective actions to ensure the issue is not repeated.
Roles and Responsibilities of a Hospital Pharmacist in Clinical Pharmacy Services
The expansion of clinical pharmacy services represents the pinnacle of advanced pharmacy integration. Clinical pharmacists spend a substantial portion of their shifts directly on the specialized medical units, functioning as embedded therapeutic consultants.
Ward Rounds Participation and Clinical Interventions
During morning interdisciplinary ward rounds, the clinical pharmacist walks alongside attending physicians, residents, and nurses. As the team discusses each patient’s progress, the pharmacist provides real-time recommendations regarding drug selection, alternative routes of administration, and duration of therapy. These real-time clinical interventions prevent delay of care and streamline treatment pathways.
Therapeutic Drug Monitoring (TDM)
Certain high-potency drugs possess an exceptionally narrow margin between therapeutic efficacy and severe systemic toxicity. Pharmacists run institutional TDM services, taking primary ownership over the dosing and serum concentration analysis of medications such as vancomycin, aminoglycosides, phenytoin, and digoxin. By applying precise pharmacokinetic equations, they calculate exact patient-specific dosages.
Antibiotic Stewardship Programs (ASP)
The rapid escalation of global antimicrobial resistance demands strict oversight. Hospital pharmacists lead institutional Antibiotic Stewardship efforts by:
- Enforcing restriction criteria on broad-spectrum carbapenems and reserve antibiotics.
- Reviewing microbiological cultures daily to “de-escalate” empirical broad-spectrum regimens to targeted, narrow-spectrum therapies.
- Monitoring and adjusting antibiotic courses for appropriate durations to avoid prolonged, resistance-inducing exposure.
Specialized Clinical Services
In large academic medical centers, clinical pharmacists specialize deeply within niche domains:
- Critical Care Pharmacy: Managing rapid-sequence intubations, vasoactive titrations, and advanced sedation protocols in the ICU.
- Oncology Pharmacy: Calculating complex body-surface-area-based chemotherapy regimens, designing antiemetic regimens, and ensuring hazardous drug handling protocols are met.
- Emergency Medicine Support: Providing immediate toxicological advice during drug overdoses and managing medication preparation during cardiac arrests.
Roles and Responsibilities of a Hospital Pharmacist in Drug Distribution Systems
An optimized clinical team cannot function without an flawless logistical backbone. The structural integrity of the drug distribution system falls squarely under the purview of hospital pharmacy operations.
Procurement and Inventory Management
The pharmacy operations management team evaluates historical drug utilization patterns, seasonal disease spikes, and budgetary allocations to procure medications efficiently. They maintain the delicate balance of preventing stockouts of critical lifesaving medications while avoiding excess capital tie-up in slow-moving stock.
Drug Storage, Preservation, and Inspection
Medications must be preserved under strict environmental conditions to retain their structural stability and potency:
- Cold Chain Logistics: Monitoring specialized medical refrigerators and freezers containing vaccines and biologicals using continuous, logged digital telemetry.
- Hazardous Drug Segregation: Isolating cytotoxic agents under negative pressure ventilation systems to prevent occupational exposure.
- Controlled Substances: Securing narcotics and psychotropics within heavy-gauge biometric safes to eliminate diversion risks.
Modern Dispensing Operations
The historical method of bulk drug delivery to nursing floors has largely been replaced by safer, highly controlled frameworks:
- Unit Dose Dispensing System: In this model, individual medications are pre-packaged, labeled with distinctive barcodes, and dispensed in single-unit doses tailored to a specific patient for a 24-hour window. This drastically reduces floor stock errors.
- Automated Dispensing Systems (ADS): Decentralized automated cabinets (e.g., Pyxis, Omnicell) are strategically stationed across hospital floors. The pharmacist electronically reviews and clears an order before a nurse can physically access the automated bin, combining instant point-of-care availability with strict pharmacist oversight.
Roles and Responsibilities of a Hospital Pharmacist in Pharmacy Operations Management
Behind the clinical and logistical workflows lies a complex business operation. Effective hospital pharmacy management requires strong administrative leadership to align the department with corporate hospital goals and regulatory expectations.
Workflow Management and Human Resources
The pharmacy director or manager oversees a large team of clinical pharmacists, operational pharmacists, and pharmacy technicians. They establish efficient workflow patterns, optimize technician-to-pharmacist ratios, and handle complex staff scheduling to ensure seamless 24/7/365 coverage for acute inpatient units.
Budget Planning and Cost Control Measures
The pharmacy department represents one of the largest ongoing operational expenditures within a healthcare institution. Pharmacists control costs through:
- Formulary Management: Negotiating purchasing contracts and driving therapeutic class substitutions (e.g., using preferred biosimilars).
- Waste Reduction Programs: Implementing strict compounding adjustments for high-cost IV medications to ensure partial vials are maximized safely.
Quality Assurance and Key Performance Indicators (KPIs)
To maintain institutional prestige and safety standards, the management team establishes and monitors specific departmental KPIs. These benchmarks are analyzed during regular quality audits and serve as critical documentation during institutional accreditation reviews by bodies such as the Joint Commission International (JCI).
Hospital Pharmacy Services Overview
To summarize how these multi-faceted duties intersect, the following comprehensive matrix outlines the core functional structures within an institutional pharmacy department:
Table 1: Roles and Responsibilities Overview
| Functional Domain | Core Responsibilities | Key Operational Objective | Target Stakeholders |
| Clinical Services | Ward rounds, TDM, ASP, specialized protocol design. | Therapeutic optimization. | Physicians, Inpatients |
| Medication Safety | RCA execution, LASA management, high-alert drug controls. | Error eradication. | Hospital Administration, Patients |
| Distribution & Logistics | Procurement, cold chain management, unit-dose packaging. | Supply chain integrity. | Nursing Staff, Central Stores |
| Operational Leadership | Budgeting, staff metrics, KPI monitoring, compliance audits. | Institutional efficiency. | Finance Teams, Accrediting Bodies |
Hospital Pharmacist’s Role in Specialized Areas
As medicine sub-specializes, hospital pharmacists must adapt their clinical focus to match the unique physiological environments of distinct patient populations.

1. Intensive Care Units (ICU) and Neonatal ICU (NICU)
In adult ICUs, the pharmacist manages highly labile patients requiring precise titrations of vasopressors, continuous renal replacement therapy (CRRT) drug adjustments, and complex parenteral nutrition (PN) compounding.
In the NICU, the setting becomes even more delicate. Neonates possess highly immature hepatic and renal clearance pathways. The neonatal pharmacist calculates personalized miligram-per-kilogram or microgram-per-kilogram dosages, avoids preservatives (such as benzyl alcohol) that can cause gasping syndromes, and oversees ultra-low-volume IV preparations.
2. Oncology Units
The oncology pharmacist ensures the absolute accuracy of hazardous chemotherapy compounding within specialized ISO Class 5 cleanrooms. They cross-check cumulative lifetime doses of cardiotoxic agents (like doxorubicin) and manage complex supportive care regimens to prevent debilitating chemotherapy-induced nausea, vomiting, and myelosuppression.
3. Emergency Departments (ED)
Time is of the essence in the ED. The emergency medicine pharmacist acts as an immediate bedside consultant during acute stroke presentations (calculating thrombolytic windows), status epilepticus, toxicological overdoses, and major trauma resuscitations. They ensure medication histories are compiled immediately to avoid omissions during urgent admissions.
4. Infectious Disease and Transplant Services
Infectious disease pharmacists oversee the institutional stewardship matrix, analyzing hospital antibiograms to track local resistance patterns. Transplant pharmacists manage lifetime immunosuppressive therapies, carefully balancing the prevention of graft rejection against the risk of opportunistic systemic infections.
Roles and Responsibilities of a Hospital Pharmacist in Patient Counseling
The clinical duty of a hospital pharmacist does not end when the medical team decides a patient is well enough to return home. Transitional care is a high-risk period for medication discrepancies.
Discharge Counseling and Medication Reconciliation
Medication reconciliation is the formal process of creating the most accurate list possible of all medications a patient is taking (including name, dosage, frequency, and route) and comparing it against the admission, transfer, and discharge orders. During discharge counseling, the pharmacist sits with the patient or caregiver to explain:
- Which pre-admission medications are being discontinued.
- The exact indications, side effects, and administration times for newly prescribed therapies.
- How to navigate complex delivery devices, such as insulin pens or dry-powder inhalers.
Improving Medication Adherence in Special Populations
Non-adherence is a major driver of preventable hospital readmissions. Pharmacists address this by simplifying complex regimens into once-daily dosing schedules where possible, coordinating with outpatient pharmacies for blister-packing, and counseling vulnerable populations. For pediatric patients, this includes calculating precise liquid volumes; for geriatric patients, it involves evaluating visual or cognitive barriers and minimizing polypharmacy.
Hospital Pharmacists and Multidisciplinary Healthcare Teams
Modern healthcare operates on interdisciplinary collaboration. The hospital pharmacist serves as the essential pharmacotherapeutic anchor within this matrix, interfacing continuously with multiple departments.

Collaborative Workflow Integrations
- With Physicians: Providing real-time drug selection advice, alternatives during shortages, and complex pharmacokinetic dosing calculations.
- With Nursing Staff: Clarifying proper Medication Administration techniques, drug compatibility profiles for co-infused IV lines, and optimal infusion rates.
- With Clinical Dietitians: Coordinating total parenteral nutrition (TPN) components to fulfill exact caloric and electrolyte demands while avoiding drug-nutrient precipitations.
- With Infection Control & Quality Teams: Developing institutional disinfection guidelines, monitoring needle-stick protocols, and designing safety initiatives to reduce hospital-acquired infections.
Technology and Digital Transformation in Hospital Pharmacy
The integration of advanced healthcare informatics has radically optimized how inpatient pharmacy services are structured. Digital workflows significantly reduce the chance of human transcription errors.
1. CPOE and Electronic Prescribing
Computerized Physician Order Entry (CPOE) eliminates the historical danger of illegible handwritten prescriptions. Pharmacists review orders directly within a digital queue, allowing them to systematically process high volumes of profiles with greater accuracy.
2. Barcode Medication Administration (BCMA)
BCMA is a major advancement in bedside safety. Every single unit-dose medication is printed with a distinct linear or 2D barcode. Before administration, the nurse scans the patient’s biometric wristband and then scans the medication barcode. The system verifies the “Five Rights” (Right Patient, Right Drug, Right Dose, Right Route, Right Time), and alerts the nurse immediately if a discrepancy occurs.
3. Clinical Decision Support Systems (CDSS) & AI
Modern pharmacy informatics packages feature embedded CDSS algorithms. When a physician or pharmacist inputs an order, the software automatically runs real-time cross-checks against the patient’s laboratory values and existing medication lists. Looking forward, the integration of Artificial Intelligence (AI) predictive modeling helps forecast local drug shortages, optimize inventory turns, and identify early physiological markers of patient sepsis based on drug utilization patterns.
Hospital Pharmacist’s Role in Regulatory Compliance
Operating an institutional pharmacy requires strict adherence to an array of local, national, and international statutes. Compliance is critical to avoid legal liability and maintain operational licenses.
1. Pharmacy Laws and Controlled Substance Regulations
Pharmacists maintain meticulous, legally mandated perpetuating logs for all schedules of controlled substances. Every single milligram of narcotic medication must be traceable from the initial wholesale invoice down to the final bedside patient administration or documented destruction site.
2. Audit Readiness and Accreditation Standards
Whether preparing for a national health inspection or a comprehensive JCI accreditation survey, the hospital pharmacist ensures that the department meets all standard operating procedures (SOPs). This includes validating cleanroom sterility certification records, confirming up-to-date staff competencies, and documenting complete refrigerator temperature logs.
Roles and Responsibilities of a Hospital Pharmacist in Education and Training
As academic centers of medical excellence, hospitals rely heavily on their pharmacy departments to cultivate the next generation of healthcare providers.
Internal and External Education Pathways
- Training Pharmacy Interns and Residents: Post-graduate residency programs (e.g., PGY1 and PGY2) are rigorously mentored by senior clinical specialists to develop advanced critical thinking and diagnostic skills.
- Nursing and Medical Staff In-Services: Pharmacists present educational updates regarding newly approved institutional drugs, modified toxicity protocols, or altered IV compatibility guidelines.
- Clinical Research and Trials Support: Hospital pharmacists manage the complex investigational drug services required for clinical trials. They ensure precise double-blind randomizations, track specific study drug storage criteria, and report unexpected investigational adverse events to institutional review boards.
Hospital Pharmacist’s Role in Emergency Preparedness
When unexpected crises hit a community, the hospital pharmacy department must ensure immediate, uninterrupted continuity of care.
Disaster and Pandemic Preparedness
During mass casualty incidents, natural disasters, or global pandemics, pharmacists are responsible for executing emergency surge protocols. They rapidly mobilize antidote stockpiles, configure mobile dispensing carts for emergency field tents, and establish allocation algorithms for critical mechanical ventilation medications during acute supply disruptions.
Proactive Drug Shortage Management
Global pharmaceutical supply chains are fragile. Hospital pharmacists spend a considerable amount of operational time tracking impending manufacturer shortfalls. When a critical front-line drug becomes unavailable, the pharmacist coordinates with clinical committees to source safe, equivalent therapeutic alternatives and updates the electronic health record systems to guide clinicians toward available options.
A Typical Day in the Life of a Hospital Pharmacist
To visualize how these diverse clinical, operational, and administrative duties weave together, let us look at a realistic daily timeline for a clinical specialist assigned to an inpatient internal medicine unit.

Shift Timeline: Internal Medicine Clinical Specialist
- 07:30 AM – 08:30 AM: Handover and Electronic Profile ReviewThe day begins by receiving handovers from the overnight pharmacy team. The pharmacist reviews the electronic dashboard, prioritizing patients newly admitted overnight, checking morning laboratory panels, and highlighting critical out-of-range lab alerts (e.g., elevated serum potassium or declining renal function).
- 08:30 AM – 11:00 AM: Multidisciplinary Ward RoundsThe pharmacist joins the medical team at the bedside. They consult on 15 to 20 acute patients, advising on empiric antibiotic selections, suggesting modifications for renal dosing, and resolving immediate medication inquiries from physicians and nurses.
- 11:00 AM – 12:30 PM: Post-Round Documentation and Targeted InterventionsReturning to the clinical station, the pharmacist documents specific therapeutic interventions within the patient health records, contacts the central compounding cleanroom to fast-track urgent IV adjustments, and processes newly generated midday medication orders.
- 12:30 PM – 01:30 PM: Lunch Break and Administrative Catch-upBrief operational downtime, followed by checking departmental communications regarding regional drug shortages or updated institutional protocols.
- 01:30 PM – 03:00 PM: Therapeutic Drug Monitoring (TDM) & Patient CounselingThe pharmacist runs kinetic calculations for vancomycin and aminoglycoside levels drawn that morning, adjusting dosages for the upcoming cycles. Afterwards, they head to the discharge ward to conduct bedside medication counseling for patients transitioning back home.
- 03:00 PM – 04:00 PM: Nursing Unit Inspections & End-of-Day HandoverThe pharmacist performs routine safety sweeps of the decentralized automated dispensing cabinets on the unit to check for proper storage and expiration dates. They then compile summary clinical handovers for the oncoming evening shift to ensure continuity of care.
Data-Driven Practice Metrics
To further illustrate the allocation of responsibilities and systemic focus within hospital pharmacy practice, the following matrices detail clinical, safe operational, and professional competencies.
Table 2: Clinical Pharmacy Services & Interventions
| Core Activity | Clinical Action | Therapeutic Target | Impact Measure |
| Therapeutic Drug Monitoring | Serum trough/peak analysis via pharmacokinetic modeling. | Narrow therapeutic index drugs (e.g., Vancomycin). | Prevention of acute kidney injury (AKI). |
| Antimicrobial Stewardship | De-escalation of empirical therapies based on culture reports. | Broad-spectrum antibiotics. | Mitigation of multidrug-resistant organisms. |
| Medication Reconciliation | Cross-checking pre-admission history with current orders. | All chronic therapies. | Prevention of post-discharge readmissions. |
Table 3: Medication Safety Activities & Interventions
| Risk Factor | Pharmacy Intervention Strategy | Safety Mechanism |
| High-Alert Medications | Mandatory independent double-checks and dedicated storage. | Human-error redundancy. |
| Look-Alike Sound-Alike (LASA) | Application of Tall Man lettering and distinct visual bin labels. | Visual cognitive differentiation. |
| Intravenous Incompatibilities | Multi-line drug compatibility mapping and reference charting. | Precipitation and inactivation prevention. |
Table 4: Specialized Hospital Pharmacy Areas
| Specialty Unit | Unique Pharmacist Responsibility | Primary Clinical Focus |
| Neonatal ICU (NICU) | Preservative-free fluid management; ultra-precise micro-dosing. | Pediatric metabolic limitations. |
| Oncology Service | BSA chemotherapy calculations; hazardous spill containment protocols. | Cytotoxic safety and accurate targeting. |
| Emergency Department | Immediate antidote selection; bedside rapid-sequence intubation prep. | Time-critical emergency resuscitations. |
Table 5: Required Skills and Competencies
| Skill Category | Specific Competency Requirement | Clinical/Operational Utility |
| Advanced Therapeutics | Deep understanding of complex Pharmacology Basics. | Authoritative clinical intervention execution. |
| Interpersonal Communication | Clear, concise verbal delivery under high-stress conditions. | Seamless multidisciplinary team integration. |
| Informatics Literacy | High proficiency in CPOE, BCMA, and electronic health registries. | Navigation of modern digital hospital ecosystems. |
Table 6: Career Progression Pathway
| Professional Tier | Typical Experience Required | Primary Focus Area |
| Staff/Operational Pharmacist | Entry-level (0–2 years) | Order verification, cleanroom compounding, dispensing. |
| Clinical Pharmacy Specialist | 2–5 years + PGY1/PGY2 Residency | Direct ward rounds, TDM, targeted disease-state intervention. |
| Clinical Coordinator / Supervisor | 5–8 years | Oversight of specialized therapeutic lines (e.g., ASP lead). |
| Director of Pharmacy Services | 8+ years + Master’s (MHA/MBA) | Macro-budgetary planning, legal liability, hospital-wide operations. |
Table 7: Common Challenges and Solutions
| Identified Operational Challenge | Root Cause Driver | Proposed Structural Solution |
| Institutional Workforce Burnout | Escalating patient acuity alongside high documentation demands. | Optimization of technician support and automated workflows. |
| Unpredictable Medication Shortages | Fragmented global manufacturing and raw material logistics. | Proactive thermodynamic alternative substitution mapping. |
| Inadvertent Medication Discrepancies | Poorly structured patient transitions between hospital units. | Expansion of dedicated transition-of-care pharmacist lines. |
Career Path and Growth Opportunities for Hospital Pharmacists
The healthcare pharmacist career offers a highly structured and rewarding trajectory for professionals dedicated to continuous learning.
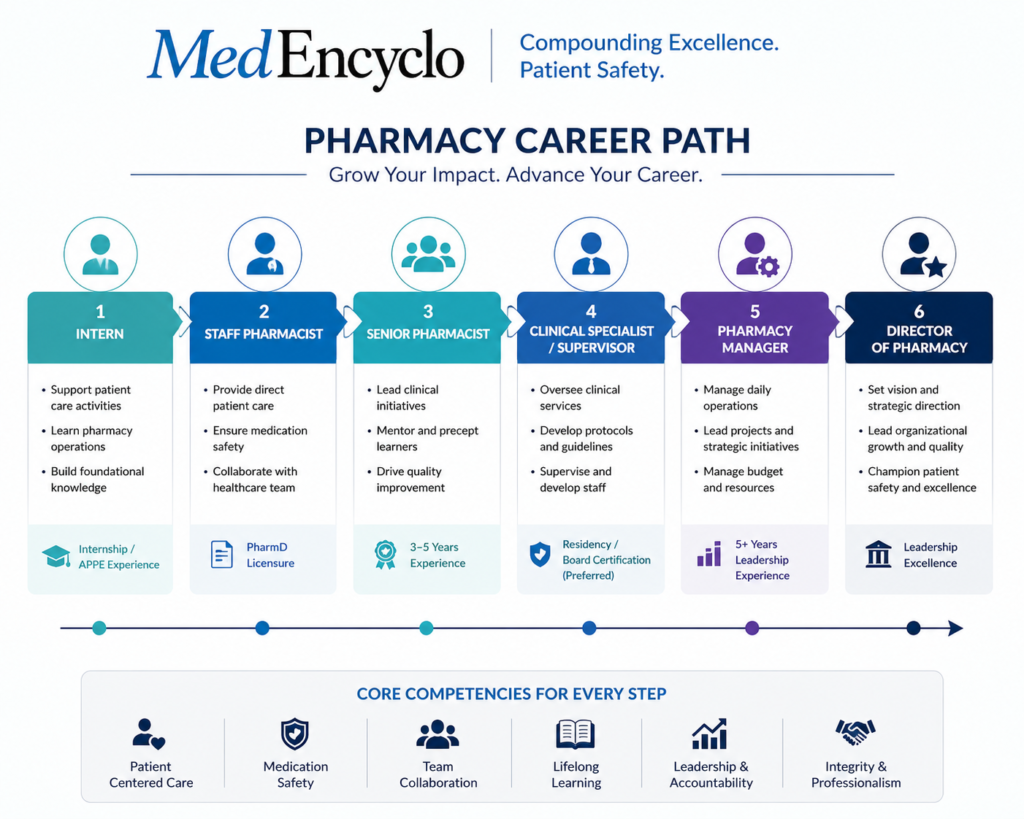
1. From Entry-Level to Executive Leadership
- Staff/Operational Pharmacist: Focusing on core drug distribution systems, compounding safety, and sterile preparation workflows.
- Clinical Pharmacist / Specialist: Transitioning into decentralized patient units, managing complex pharmacotherapy regimens, and driving clinical outcomes.
- Pharmacy Manager / Clinical Coordinator: Overseeing designated functional sub-departments, establishing therapeutic protocols, and managing staff allocations.
- Director of Pharmacy / Chief Pharmacy Officer: Operating at the executive leadership level, managing multi-million dollar budgets, shaping institutional clinical policies, and interacting directly with hospital board members.
2. Post-Graduate Residency and Fellowship Specialization
To advance rapidly within modern clinical environments, graduates frequently pursue Post-Graduate Year 1 (PGY1) residencies, which focus on generalized institutional practice, followed by Post-Graduate Year 2 (PGY2) residencies for deep specialization in fields such as cardiology, solid organ transplantation, critical care, or pharmacy informatics.
Skills Required to Become a Successful Hospital Pharmacist
Succeeding in this challenging, fast-paced environment requires a balanced mix of advanced cognitive knowledge and strong interpersonal skills.
- Clinical Acumen: Maintaining an exhaustive, up-to-date knowledge base regarding complex pharmacokinetics, multi-disease pathophysiology, and emerging drug entities.
- Effective Communication: The ability to articulate complex pharmacological concepts clearly to a physician under intense time pressure during a code blue, or to explain a medication schedule empatheticly to an anxious patient at discharge.
- Problem-Solving and Adaptability: Rapidly evaluating therapeutic alternatives when front-line drugs are unavailable due to unexpected supply chain disruptions.
- Technological Literacy: Seamlessly navigating advanced clinical software, smart pump telemetry, and modern database frameworks.
Challenges Faced by Hospital Pharmacists
While the profession is highly rewarding, hospital pharmacists operate under unique systemic pressures that require resilience and strategic planning.
1. Supply Shortages and Increasing Patient Complexity
Managing chronic manufacturing shortages requires a significant amount of administrative time. Compounding this challenge is an aging inpatient population presenting with multiple chronic comorbidities, which drastically increases the risk of Drug Safety & Interactions.
2. Workload and Burnout Management
Operating within a high-stakes, 24/7 clinical environment can lead to professional burnout. Hospital administrations are actively addressing this by expanding the utilization of advanced pharmacy technicians to handle operational tasks, freeing clinical pharmacists to focus on direct patient-centered care.
Real-Life Case Studies
To demonstrate the practical value of a hospital pharmacist, the following real-world scenarios highlight clinical interventions across various hospital units.
Case Study 1: Medication Error Prevention
- Situation: An attending physician accidentally entered an order for intravenous methotrexate daily instead of the indicated weekly dosing schedule for an elderly patient with severe rheumatoid arthritis admitted for an unrelated infection.
- Pharmacist Action: During the computerized prescription verification process, the clinical pharmacist immediately caught the daily ordering frequency. Recognizing that daily administration of oncology-dose methotrexate causes catastrophic, fatal bone marrow suppression, the pharmacist put an immediate hold on the order and contacted the prescriber.
- Outcome: The physician realized the automated entry error, thanked the pharmacist, and corrected the order to a weekly cycle.
- Lesson Learned: Automated electronic system drop-downs can inadvertently cause selection slips. Experienced clinical verification remains a vital safety layer.
Case Study 2: Clinical Intervention in Critical Care
- Situation: A patient in the ICU with severe septic shock was showing signs of worsening acute kidney injury (AKI). The patient was receiving continuous infusions of vancomycin for suspected MRSA bacteremia.
- Pharmacist Action: The critical care pharmacist reviewed the morning lab results and noted a sharp rise in serum creatinine alongside falling urine output. The pharmacist halted the scheduled vancomycin dose, ordered an immediate random serum vancomycin trough level, and calculated a revised dosing interval based on altered renal clearance models.
- Outcome: The random trough level came back high ($32\ \mu\text{g/mL}$). The pharmacist safely withheld further doses until the drug cleared to a safe therapeutic range, preventing further drug-induced nephrotoxicity.
- Lesson Learned: Dynamic, real-time monitoring of organ function is critical when administering narrow therapeutic index drugs to unstable patients.
Case Study 3: Drug Interaction Management
- Situation: A patient with a mechanical heart valve on a stable, long-term maintenance dose of warfarin was admitted with a severe atypical pneumonia and started on intravenous erythromycin.
- Pharmacist Action: The ward pharmacist recognized that erythromycin is a potent inhibitor of hepatic CYP1A2 and CYP3A4 enzymes, which are responsible for metabolizing warfarin. This interaction would cause the patient’s International Normalized Ratio (INR) to spike, putting them at extreme risk for a life-threatening hemorrhage.
- Outcome: The pharmacist intervened, advising the medical team to switch erythromycin to an alternative antibiotic with minimal CYP450 involvement (such as azithromycin) and scheduled additional INR monitoring. The patient remained safe and stable.
- Lesson Learned: Thorough screening for Adverse Drug Reactions and drug interactions prevents serious, preventable complications.
Case Study 4: Antibiotic Stewardship Program Success
- Situation: An orthopedic patient post-surgery was started on empirical intravenous meropenem—a powerful, broad-spectrum carbapenem—for a suspected surgical site infection.
- Pharmacist Action: On day three of therapy, the infectious disease pharmacist reviewed the wound culture microbiology reports, which came back positive for highly sensitive Staphylococcus aureus. The pharmacist contacted the surgical team to recommend de-escalating from the broad-spectrum carbapenem to a targeted course of intravenous cefazolin.
- Outcome: The team accepted the recommendation. The patient’s infection cleared successfully, and the hospital avoided unnecessary broad-spectrum antibiotic exposure.
- Lesson Learned: Targeted antibiotic de-escalation effectively cures infections while preserving the efficacy of critical broad-spectrum agents.
Case Study 5: Patient Counseling Success Story
- Situation: A 72-year-old patient with a history of recurrent heart failure hospitalizations was being discharged on a newly adjusted regimen that included a complex diuretic schedule and a new anticoagulant.
- Pharmacist Action: The transition-of-care pharmacist conducted an in-depth bedside discharge counseling session. During the review, the pharmacist discovered that the patient lived alone, had poor eyesight, and was confused about how to differentiate their old medications from the new prescriptions. The pharmacist prepared a personalized, high-visibility medication schedule and arranged for the local community pharmacy to supply the medications in pre-sorted blister packs.
- Outcome: The patient clearly understood the updated routine, remained adherent, and did not experience a re-hospitalization at the 30-day follow-up mark.
- Lesson Learned: Comprehensive patient education at discharge bridges the gap between clinical treatment and long-term recovery at home.
Future of Hospital Pharmacy Practice
The practice of hospital pharmacy is positioned for exciting growth as healthcare models become more precise and integrated.
1. Precision Medicine and Pharmacogenomics
As genomic sequencing becomes a standard part of diagnostic medicine, hospital pharmacists are leading the clinical rollout of pharmacogenomics. By analyzing a patient’s specific genetic profile, pharmacists can predict how they will metabolize certain drugs, allowing them to select the most effective medication at the correct dose from the very start.
2. Telepharmacy and Expanded Digital Health
The expansion of telepharmacy allows specialized clinical pharmacists to provide remote clinical review, TDM calculations, and verification services to small rural hospitals that may not have full-time clinical specialists on site. This ensures that high-quality pharmaceutical care is accessible to all patients, regardless of geography.
Frequently Asked Questions (FAQ)
What does a hospital pharmacist do?
A hospital pharmacist manages the selection, verification, compounding, storage, and dispensing of medications within an institutional setting. They collaborate closely with doctors and nurses, participate in clinical ward rounds, perform therapeutic drug monitoring, and run medication safety initiatives to optimize inpatient care.
How is hospital pharmacy different from retail pharmacy?
Hospital pharmacy practice is embedded within acute institutional environments, focusing on complex multi-disease clinical management, intravenous compounding, and direct interdisciplinary teamwork. Retail pharmacy operates in accessible community locations, focusing on outpatient dispensing, retail operations, and general public health counseling.
Can hospital pharmacists prescribe medications?
Prescribing privileges vary by jurisdiction and country. In many modern healthcare systems, qualified clinical pharmacists possess collaborative prescribing rights. This allows them to independently adjust dosages, order relevant laboratory tests, and manage specific therapeutic lines under an institutional protocol agreed upon with physicians.
What qualifications are required to become a hospital pharmacist?
Professionals must earn a professional pharmacy degree (such as a PharmD or BPharm depending on the country), clear national licensing board examinations, and obtain a valid registration to practice. Many clinical positions require an additional one to two years of accredited post-graduate residency training.
What are the biggest responsibilities of a hospital pharmacist?
The core responsibilities include verifying the clinical appropriateness of all medication orders, preventing harmful drug interactions, executing precise therapeutic drug monitoring, maintaining secure drug supply chains, and managing medication safety workflows to eliminate clinical errors.
What is therapeutic drug monitoring (TDM)?
TDM is the clinical practice of measuring serum drug concentrations to personalize medication dosing. Pharmacists use these levels to ensure that medications with narrow therapeutic windows are effective without causing systemic toxicity.
How do pharmacists prevent Look-Alike Sound-Alike (LASA) errors?
They use strategies like Tall Man Lettering to highlight differences in drug names on electronic screens, physically separate similarly packaged medications on pharmacy shelves, and utilize barcode confirmation workflows before dispensing.
Key Takeaways
- Clinical Evolution: The roles and responsibilities of a hospital pharmacist have advanced into a highly clinical, patient-centered discipline essential to modern healthcare teams.
- Medication Safety Champions: Pharmacists provide critical safety checks, managing high-alert drugs and using strategies like Tall Man Lettering to prevent clinical errors.
- Direct Inpatient Integration: Embedded clinical specialists participate in ward rounds, run TDM services, and lead antibiotic stewardship programs to improve patient outcomes.
- Operational Excellence: The department manages complex logistical workflows, including cold chain storage and unit-dose dispensing, to keep the hospital supply chain safe and efficient.
- Transition of Care Leaders: Through careful medication reconciliation and clear discharge counseling, pharmacists protect patients during the critical transition from hospital to home.
Conclusion
The modern hospital pharmacist is a vital clinical strategist, a safety expert, and an essential partner on the multidisciplinary healthcare team. As the complexity of medicine continues to grow, their role in managing medications safely and effectively becomes even more critical to institutional healthcare quality. By combining deep clinical knowledge with operational expertise, hospital pharmacists protect patient safety and ensure that modern medicine is delivered with precision and care.
References
- American Society of Health-System Pharmacists (ASHP). ASHP Guidelines on Pharmacy-Led Medication Reconciliation.
- World Health Organization (WHO). The Role of the Pharmacist in the Health Care System.
- Institute for Safe Medication Practices (ISMP). High-Alert Medications in Acute Care Settings.
- Centers for Disease Control and Prevention (CDC). The Core Elements of Hospital Antibiotic Stewardship Programs.
“This content is for informational and educational purposes only and is not intended as medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any medical decisions.”