Imagine driving down a busy metropolitan highway or a bustling intersection when a sudden, sickening crunch of metal echoing through the air shatters the peace. A car has veered off course, colliding head-on with a motorcycle before skidding into a concrete divider. Smoke rises from the crushed hoods, traffic grinds to a halt, and you hear faint cries for help.
As a bystander, your heart pounds wildly, your adrenaline surges, and panic threatens to freeze your actions. In this exact moment, you are the most critical link in the survival chain. The actions you take in the next ten minutes can mean the difference between life and permanent disability, or even life and death.
When major trauma occurs on the road, knowing the fundamentals of Road Traffic Accidents First Aid can turn a terrified onlooker into a capable lifesaver. This guide provides an exhaustive, trauma-specialist-approved framework to stabilize victims and manage the scene safely until professional paramedics arrive.
Understanding Road Traffic Accidents and Emergency Response
When a vehicle traveling at high speeds suddenly stops, the human body inside experiences intense, violent forces. This deceleration transfers massive kinetic energy directly to internal organs, bones, and soft tissues, leading to complex trauma patterns.
[Vehicle Collision] ──> [Rapid Deceleration] ──> [Kinetic Energy Transfer] ──> [Multi-System Trauma]
In emergency medicine, we emphasize the concept of the “Golden Hour.” This refers to the critical 60-minute window immediately following a severe traumatic injury.
- The Critical Window: If a victim with severe internal or external bleeding receives definitive surgical care within this hour, their chances of survival increase exponentially.
- The Platinum Ten Minutes: The first 10 minutes of that hour belong entirely to you, the bystander or first responder. Paramedics cannot materialize instantly, meaning your immediate actions directly combat early death from airway blockages or massive blood loss.
- The Reality of Road Trauma: According to data from the World Health Organization (WHO), millions of lives are lost globally each year to road traffic injuries, with a staggering percentage occurring due to lack of immediate, on-scene stabilization.
By mastering basic Road Accident First Aid, you act as the bridge between the moment of impact and advanced clinical trauma care. You do not need a medical degree to save a life; you simply need a systematic, structured plan.

Road Traffic Accidents First Aid – Priorities Before Helping
Before you rush toward a crumpled vehicle to pull a victim out, you must pause and assess the environment. An injured or dead first responder cannot save anyone else, and adding another casualty to the scene only stretches arriving emergency resources thinner.
Personal Safety First
Your safety is the absolute non-negotiable priority at any accident scene. Take a deep breath, look around, and ensure that stepping into the roadway will not result in you being hit by oncoming traffic or exposed to chemical hazards.
Scene Assessment
Perform a rapid visual sweep of the area within a 50-meter radius. You must look for and identify several high-risk physical threats:
- Traffic Hazards: Are other vehicles approaching at high speeds, blind bends, or low-visibility conditions like heavy fog or rain?
- Fire Hazards and Fuel Leaks: Do you smell gasoline or diesel? Is there visible smoke, sparking electrical wires, or leaking fluids pooling under the undercarriage?
- Electrical Hazards: Are there snapped utility poles or downed power lines touching the vehicles or lying across the wet tarmac?
- Crowd Management: Is a crowd of onlookers blocking access or panicking the victims? You must firmly delegate tasks to bystanders to gain control of the space.
Road Traffic Accidents First Aid – Step 1: Ensure Scene Safety
Once you commit to helping, you must actively secure the physical environment. Never assume that other drivers can see the crash or see you.
Securing the Physical Environment
- Park Safely: If you are driving, park your own vehicle a safe distance before the accident scene (ideally 30 meters away). Turn on your hazard warning lights to act as an early warning shield for oncoming traffic.
- Deploy Warning Devices: Put on a high-visibility reflective vest if you have one. Place reflective warning triangles on the road well ahead of the scene—about 50 meters back on standard city roads, and up to 150 meters back on high-speed expressways or highways.
- Turn Off Ignitions: Approach the crashed vehicles carefully. If safe to do so, reach inside and turn off the ignitions of the damaged vehicles to eliminate engine heat and spark sources. Pull the handbrake to prevent any unexpected rolling or shifting of the chassis.
- Manage Moving Traffic: If multiple bystanders are present, explicitly instruct one or two people to stand safely on the shoulder and wave down oncoming vehicles, directing them to slow down and divert smoothly around the impact zone.
Road Traffic Accidents First Aid – Step 2: Call Emergency Services Immediately
Never assume that someone else has already called for professional medical help. The moment the scene is safe to approach, emergency dispatchers must be notified.
Activating the Local Emergency Network
- In India: Immediately dial 112, the unified single emergency response number for ambulance, police, and fire services. Alternatively, you can dial 102 for national ambulance services or 1033 for dedicated National Highway Authority of India (NHAI) trauma support on major toll ways.
- Globally: Ensure you know the local emergency codes, such as 911 in North America, 999 in the United Kingdom, or 112 across the European Union.
Delivering High-Value Dispatch Information
When speaking to the emergency operator, remain calm, speak clearly, and deliver the specific clinical and logistical details they need to route the correct trauma resources:
| Information Category | Specific Details to Provide |
| Exact Location | Landmark buildings, highway kilometer markers, intersection names, GPS coordinates, or lane directions (e.g., “Northbound lane, 2 kilometers past Exit 4”). |
| Incident Nature | Type of vehicles involved (e.g., a truck and a passenger hatchback, a pedestrian struck by a city bus). |
| Hazards Present | Leaking fuel, active fire, downed high-voltage power lines, or structural entrapment. |
| Number of Victims | A raw estimate of how many people are injured, trapped, or ejected onto the roadway. |
| Severity of Injury | Clarify if any victims are unresponsive, bleeding profusely from major wounds, or showing signs of altered breathing patterns. |
Critical Dispatch Rule: Never hang up the phone until the emergency dispatcher explicitly tells you to do so. They may provide live, step-by-step coaching for CPR or bleeding control tailored to the situation.
Road Traffic Accidents First Aid – Step 3: Rapidly Assess the Victim
When you approach the casualties, you must run through a rapid, highly structured evaluation sequence. In trauma medicine, we use the Primary Survey framework to detect and treat injuries in order of what kills a human being first.
[Responsiveness] ──> [Airway Status] ──> [Breathing Pattern] ──> [Bleeding / Circulation]
The Initial Contact Sequence
- Check for Responsiveness: Stand directly in front of the victim so they do not have to turn their head, which could damage an injured spine. Shout loudly: “Hello! Can you hear me? Open your eyes!”
- Squeeze the Shoulders: Gently but firmly squeeze their shoulder muscles. Look for any purposeful movement, eye-opening, groaning, or withdrawal from the stimulus.
- Establish Consciousness Status: Instantly categorize the victim based on their reaction. Are they fully alert and talking coherently, or are they completely limp and unresponsive to your touch and voice?
- Observe Visible Traumas: Look from head to toe for massive, spurting blood pools, unusual limb positioning, facial smash injuries, or chest movements that signal deep structural damage.
Road Traffic Accidents First Aid – Step 4: Check for Life-Threatening Conditions
To prevent premature death on the roadside, you must systematically screen for the “Fatal Triad” of trauma: airway occlusion, respiratory failure, and catastrophic external hemorrhage.
The Life-Threatening Priority Hierarchy
- Catastrophic Hemorrhage: If you see bright red blood spurting vigorously or soaking through clothing rapidly, this takes precedence even over airway management in modern first responder protocols (often called the C-ABC approach). Stop this bleeding instantly.
- Airway Problems: If the airway is blocked by a slumped tongue, fractured facial bones, thick blood clots, or vomit, the brain will suffer irreversible hypoxic injury (lack of oxygen) within 4 to 6 minutes.
- Breathing Problems: Is the chest rising and falling symmetrically? Is the victim gasping for air like a fish out of water, or is their chest wall moving abnormally?
- Cardiac Arrest: If the heart has stopped beating due to extreme physical impact or severe lack of oxygen, blood flow to the brain stops entirely.
- Unconsciousness: Deeply unconscious victims lose their natural airway protective reflexes, meaning their tongue can slide backward and choke them to death silently.
Road Traffic Accidents First Aid – Step 5: Protect the Airway
An open, clear airway is the absolute baseline of human life. If oxygen cannot enter the lungs, no other first aid intervention will save the victim.
Managing Airway Obstructions
If a victim is unconscious or deeply dazed, their tongue can sag backward into the pharynx (throat), functioning as an anatomical plug. Alternatively, shattered teeth, loose dentures, vomit, or pooled blood can completely block the respiratory passage.

Executing Airway Maneuvers Properly
- The Jaw-Thrust Maneuver (Preferred in Trauma): If you suspect a neck or spine injury, do not tilt the head back. Instead, kneel behind the victim’s head. Place your fingers behind the angles of their lower jawbone and gently push the jaw upward and forward. This pulls the tongue away from the back of the throat without bending the neck.
- The Head-Tilt, Chin-Lift Maneuver: Use this only if you cannot open the airway with a jaw-thrust and the victim is suffocating. Place one hand on the forehead, apply gentle backward pressure, and lift the bony tip of the chin with your index and middle fingers.
- Clearing Fluids: If the mouth is filled with vomit or blood, gently roll the victim’s entire body as a single, coordinated unit (log-rolling) onto their side to let gravity drain the fluids out of the mouth, preventing aspiration into the lungs. Keep the head, neck, and torso aligned throughout the turn.
Road Traffic Accidents First Aid – Step 6: Check Breathing
Once the airway path is open and clear, you must determine if the lungs are functioning well enough to oxygenate the vital organs.
Assessing the Quality of Respiration
Place your ear close to the victim’s mouth and nose while looking down at their chest wall. Spend a full 10 seconds executing these three assessment actions:
- Look: See if the chest rises and falls rhythmically.
- Listen: Hear the sound of air escaping during exhalation.
- Feel: Sense the warmth of the breath against your cheek.
Identifying Abnormal Breathing Patterns
- Normal Respiration: Smooth, regular chest rise between 12 and 20 times per minute for an adult.
- Respiratory Distress: Rapid, shallow breaths, panting, or using neck muscles to pull air in.
- Agonal Breathing: Snorting, heavy gasping, or irregular moaning sounds that happen at long intervals.
Clinical Warning on Agonal Breathing: Agonal gasping is not effective breathing. It is a neurological reflex that occurs when the brain is actively dying from cardiac arrest. If you observe agonal breathing, treat the victim as if they are not breathing at all and prepare for immediate resuscitation.
Road Traffic Accidents First Aid – Step 7: Start CPR if Necessary
If your assessment shows that the victim is completely unresponsive and either not breathing at all or only showing agonal gasping, their heart has stopped. You must begin cardiopulmonary resuscitation (CPR) instantly to manually pump blood to their brain and vital organs.
Step-by-Step Emergency CPR Guide
- Position the Victim: Ensure the victim is lying flat on their back on a hard, level surface like the road surface or floor. Do not perform compressions on a soft car seat.
- Hand Placement: Place the heel of one hand directly on the center of the victim’s chest, right on the lower half of the breastbone (sternum). Interlock your fingers of the other hand on top, keeping your fingers pulled up so they do not press on the ribs.
- Body Alignment: Position your shoulders directly over your hands, lock your elbows completely straight, and use your upper body weight to drive straight down.
- Compression Depth: Compress the chest firmly to a depth of at least 5 centimeters (2 inches), but no more than 6 centimeters, allowing the chest to rebound completely after each push.
- Compression Rate: Pump at a rapid rhythm of 100 to 120 compressions per minute.
- The CPR Cycle: Alternate 30 high-quality chest compressions followed by 2 quick rescue breaths (if you are trained and willing to perform mouth-to-mouth). If you do not have a barrier mask or feel uncomfortable with rescue breaths, perform Hands-Only CPR—continuous, uninterrupted chest compressions.
- Utilize an AED: If a bystander can locate an Automated External Defibrillator (AED) from a nearby public space or emergency vehicle, turn it on and follow its spoken voice instructions immediately.

Road Traffic Accidents First Aid – Step 8: Control Severe Bleeding
Exsanguination—bleeding to death—is the single most common cause of preventable death following road traffic accidents. An adult can bleed to death from a severed major artery in under 3 minutes. Stopping external blood loss must be done immediately.
Methods for Managing Hemorrhage
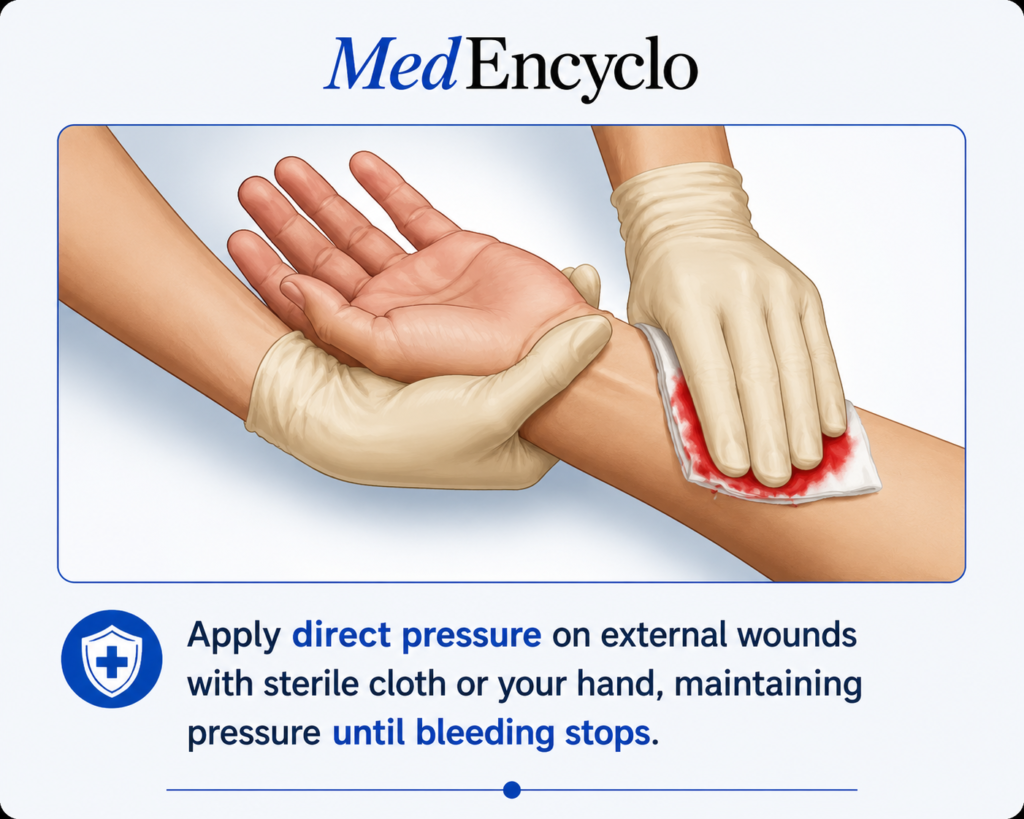
Direct Pressure
This is your primary and most effective defensive measure. Place a clean, sterile gauze pad, a thick sanitary pad, or a rolled-up clean cotton cloth directly over the weeping wound. Lean forward and apply heavy, continuous downward force using the heels of your hands. Maintain this unbroken pressure for at least 5 to 10 minutes without lifting your hands to check if the bleeding has stopped.
Pressure Dressings
Secure your clean packing material firmly in place by wrapping an elastic or cotton roller bandage tightly over the wound site. The wrap must be snug enough to maintain constant pressure on the ruptured blood vessels, but not so tight that it turns the skin below blue or obliterates the pulse.
Wound Packing
For deep, gaping lacerations or tears located in junctional body regions like the groin or the armpit where traditional bandages cannot apply enough force, push clean gauze or cotton cloth directly into the cavity of the wound. Pack it in tightly layer by layer until the wound is completely packed, then hold heavy direct pressure over the top.
Tourniquet Use
If an arm or leg is partially severed, crushed, or bleeding heavily with bright red blood spurting out, and direct pressure cannot slow it down, apply a mechanical tourniquet immediately:
- Place the band approximately 2 to 3 inches above the bleeding wound site, directly on the bare skin (never over a joint).
- Tighten the windlass rod firmly until the bright red spurting stops completely and the distal pulse disappears.
- Secure the rod in place and clearly write down the exact time of application on the tourniquet or the victim’s forehead. Never cover a tourniquet with clothing, so arriving doctors can spot it instantly.
Warning Signs of Hidden Internal Bleeding
Not all blood loss is visible. Violent impact can cause massive bleeding inside the chest, abdomen, or pelvic cavities. Watch for these subtle clinical signs:
- Coughed-up bright red, frothy blood or dark vomit resembling coffee grounds.
- Progressive bruising developing across the abdominal wall or flanks.
- Cold, pale, clammy skin matched with an incredibly fast, weak pulse.
- Rigid, stiff, or distended abdominal muscles that are painful to the touch.
Road Traffic Accidents First Aid – Step 9: Manage Shock
In trauma care, medical shock refers to hypovolemic shock—a systemic, life-threatening drop in blood pressure that happens when the organs do not receive enough oxygen-rich blood flow due to severe fluid loss.
Spotting the Progressive Signs of Shock
| Assessment Metric | Early Shock Symptoms | Advanced Shock Symptoms |
| Mental State | Mild anxiety, restlessness, or a feeling of impending doom. | Severe confusion, extreme lethargy, slurred words, or unconsciousness. |
| Heart Rate | Elevated pulse rate (tachycardia) above 100 beats per minute. | Weak, thready, irregular pulse that feels difficult to locate at the wrist. |
| Skin Signs | Mild paleness, slight cool touch to the fingertips. | Ash-gray or bluish lips and nail beds (cyanosis), cold sweat covering the body. |
| Respiration | Slightly increased breathing rate. | Rapid, shallow, labored breathing or gasping for air. |
First Aid Protocol for Combating Shock
- Positioning: Lay the victim flat on their back on a hard surface if their injuries allow it. If you are confident there are no spinal, pelvic, or lower limb fractures, elevate their legs about 12 inches (30 centimeters) off the ground to help pool blood back toward the heart and brain.
- Thermal Regulation: Traumatic shock impairs the body’s natural temperature control mechanisms, and hypothermia dramatically worsens blood clotting performance. Wrap the victim completely in a warm blanket, heavy jacket, or emergency space blanket. Insulate them from the cold asphalt below.
- Loosen Tight Clothing: Undo tight collars, neckties, belts, or restrictive clothing around the neck and chest to support unhindered respiration and circulation.
Road Traffic Accidents First Aid – Step 10: Suspected Head Injuries
High-velocity impact routinely forces the soft tissue of the brain to slam violently against the hard interior walls of the skull, causing concussions, contusions, or intracranial hematomas (internal bleeding inside the skull).
Evaluating Brain Trauma
- Concussion Identifiers: Temporary loss of consciousness, repetitive questioning, dizziness, severe nausea, vomiting, or memory gaps regarding the crash details.
- Physical Skull Disruptions: Look for deep lacerations on the scalp, visible depressions or indentations in the skull bones, or bruising around both eyes (known clinically as “raccoon eyes”).
- The CSF Indicator: Look closely for any clear, watery fluid mixed with blood leaking out of the ears or nose. This fluid is cerebrospinal fluid (CSF), and its presence confirms a serious tear in the protective membranes surrounding the brain, often indicating a basilar skull fracture.
[Blunt Head Impact] ──> [Brain Displacement] ──> [Membrane Tear] ──> [CSF Leakage from Ears/Nose]
Critical Rules for Managing Cranial Trauma
- Keep Head Neutral: If the victim is conscious, instruct them to lie completely still. Do not let them shake their head to “clear their vision.”
- Avoid Plugging Leaks: If fluid or blood is actively draining from the ears or nose, do not pack them with gauze or cotton plugs. Doing so causes fluid pressure to back up into the cranium. Instead, loosely drape a sterile dressing over the ear or nose to absorb the drainage cleanly.
- Manage Scalp Bleeding Carefully: Scalp wounds bleed heavily because the scalp is packed with blood vessels. Apply direct pressure around the edges of the wound if you suspect an underlying skull fracture, rather than pushing directly down into a soft, unstable bone defect.
Road Traffic Accidents First Aid – Step 11: Suspected Neck and Spine Injuries
Unstabilized spinal cord injuries can cause irreversible, permanent paralysis or death if a bone fragment severs the spinal cord during movement. You must assume that every victim involved in a high-speed car crash or motorcycle ejection has an unstable spinal injury until proven otherwise by x-rays.
Clinical Triggers for Spinal Precautions
- The victim complains of intense, localized pain or a burning sensation along the neck, spine, or lower back.
- Numbness, tingling, or a “pins-and-needles” sensation radiating down into their hands, fingers, legs, or feet.
- Inability to independently move their fingers, wave their hands, or flex their toes.
- The victim is completely unconscious after a high-energy collision, meaning they cannot report pain or neurological symptoms to you.
Executing Spine Immobilization Effectively
- Manual In-Line Stabilization: Kneel directly behind the victim’s head. Place your hands firmly on both sides of their jaw and head. Hold the head completely still in a neutral position, in line with the rest of the spine. Act as a human brace so they cannot look left or right.
- Verbal Reinforcement: Speak calmly to the victim: “You’ve been in an accident. I am holding your head still to protect your neck. Please do not try to nod or shake your head to answer me; simply speak ‘yes’ or ‘no’.”
- Avoid Splinting with Objects: Do not try to construct a makeshift neck collar out of rolled towels or cardboard unless you are formally trained in cervical collar sizing, as poorly fitting devices can hyperextend the neck and worsen spinal cord compression.
Road Traffic Accidents First Aid – Step 12: Fractures and Broken Bones
The impact forces of a crash frequently crack or splinter long bones like the femur (thigh bone), tibia (shin bone), or humerus (upper arm bone). Fractures can be intensely painful and lead to severe internal blood loss.
Distinguishing Fracture Subtypes
- Closed Fractures: The bone is broken inside, but the surrounding skin remains intact. You will see obvious deformity, localized swelling, bruising, and severe pain when touched.
- Open Fractures: The broken, jagged ends of the bone have sliced completely through the skin layer, or an external force has torn open a path down to the fracture site. The bone may be visible in the wound, creating a high risk of deep bone infection and heavy bleeding.
Practical Stabilization Steps
- Leave the Bone Alone: Never attempt to push a protruding bone fragment back underneath the skin. Do not attempt to straighten a deformed, twisted limb. Splint the limb exactly in the position you found it.
- Manage Open Wounds First: Carefully drape a clean, moist sterile dressing over any exposed bone fragments and open wounds before applying stabilization materials.
- Immobilize the Joints: If you must apply a splint because help is hours away, use a rigid object like a thick rolled newspaper, straight tree branch, or stiff cardboard. Secure the splint to the limb using cloth strips or bandages. The splint must be long enough to immobilize the joint immediately above the break and the joint safely below the break.
Road Traffic Accidents First Aid – Step 13: Burns After Vehicle Accidents
Vehicle fires, exploding radiators, ruptured fuel lines, and deploying airbags can cause severe thermal, chemical, or electrical burns to vehicle occupants.
Categorizing and Treating Crash Burns
Thermal Burns (Flame and Heat)
- Instantly extinguish any active flames on clothing using the “Stop, Drop, and Roll” method or by smothering the fire with a heavy wool blanket.
- Cool the burn site immediately using large volumes of clean, cool running tap water for at least 10 to 20 minutes. This pulls heat out of the tissues and stops the burning process.
- Never apply ice, ice water, butter, oils, or traditional home ointments to a burn wound, as these trap heat inside the skin and worsen tissue death.
- Loosely cover the cooled area with clean plastic cling wrap or a sterile non-stick pad to shield exposed nerve endings from the air.
Chemical Burns (Battery Acid, Coolant, and Airbag Residue)
- Airbags deploy using a rapid chemical reaction that leaves behind a caustic alkaline powder dust.
- Brush any dry chemical dust off the skin using a gloved hand or cloth before rinsing.
- Flush the affected skin or eyes with continuous amounts of clean water for at least 20 minutes to completely dilute the corrosive chemical.
Road Traffic Accidents First Aid – Step 14: Caring for Unconscious Victims
An unconscious victim who is breathing normally presents a unique challenge: they are stable for now, but their airway can become blocked at any second if their position changes or if they begin to vomit.
Continuous Monitoring Protocols
- The Spinal Rule Check: If you suspect a neck or back injury, do not move the victim unless their life is threatened by immediate danger like a vehicle fire. Keep them flat, maintain manual head stabilization, and monitor their breathing every 30 seconds.
- The Lateral Recovery Position: If the victim is breathing normally, has no signs of spinal or pelvic trauma, and you must leave them to help someone else or call for help, gently roll them onto their side into the Recovery Position. This keeps their airway open and allows fluids to drain freely onto the ground.
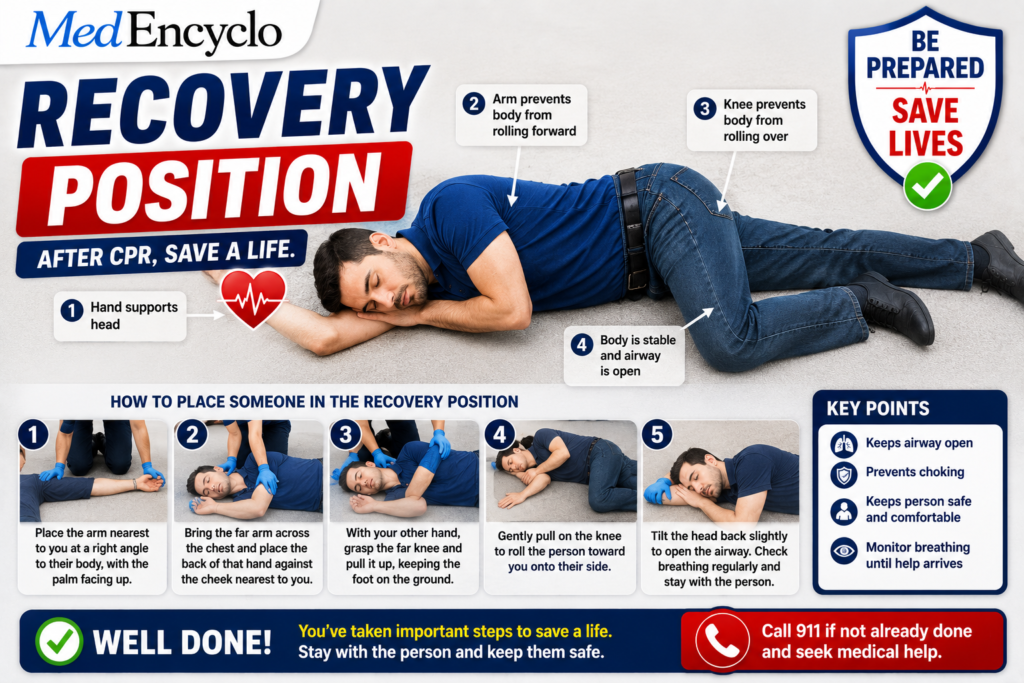
- Maintain Spinal Alignment During Roll: If you must roll an unconscious victim who might have a spinal injury because they are choking on fluids, recruit 3 to 4 bystanders to perform a synchronized Log-Roll. One person commands the head, while the others roll the shoulders, hips, and legs in unison, keeping the entire spine perfectly straight like a log.
Road Traffic Accidents First Aid – Step 15: Monitor Until Ambulance Arrives
Your first aid response does not end once you have bandaged a wound or completed initial checks. A trauma victim’s physical condition can deteriorate rapidly within minutes.
The Maintenance and Reassessment Phase
- Provide Psychological First Aid: If the victim is conscious, they will be in a state of terror and shock. Kneel beside them, maintain eye contact, and speak in a calm, reassuring voice. Say: “My name is [Name], and I’m here to help you. The ambulance has been called and is on the way. Try to take slow, deep breaths. You are not alone.”
- Recheck Vitals Constantly: Every 2 to 3 minutes, re-verify that the airway remains clear, the chest is rising normally, and applied bleeding control bandages have not soaked through.
- Gather Critical Information: If the victim is lucid, ask them key health questions using the SAMPLE framework and write down their answers:
S - Signs & Symptoms (What hurts?)
A - Allergies (Are they allergic to any medications?)
M - Medications (Do they take blood thinners or insulin?)
P - Past Medical History (Do they have a heart condition?)
L - Last Oral Intake (When did they last eat or drink?)
E - Events Leading Up (What happened right before the crash?)The Professional Handover
When the ambulance team arrives, do not simply walk away. Approach the lead paramedic or doctor and deliver a structured clinical handover:
“This is a 35-year-old male driver involved in a head-on collision. He was initially unresponsive but is now alert. He has severe bleeding from a laceration on his right thigh that I controlled using direct pressure and a compression bandage applied 10 minutes ago. He complains of severe lower back pain and shortness of breath. His breathing is currently regular at 18 breaths per minute.”
Victim Extraction – When You Should and Should Not Move Someone
One of the most dangerous and common mistakes made by well-meaning bystanders is pulling an injured person out of a crashed vehicle. Movement can turn a stable spinal fracture into a permanent spinal cord transection, resulting in instant quadriplegia.
[Unnecessary Movement] ──> [Spinal Bone Shifting] ──> [Cord Transection] ──> [Permanent Paralysis]
The Strict Extraction Standard
- When You MUST Leave Them Inside: If the vehicle is stable, there is no threat of fire, and the victim is breathing normally, leave them exactly where they are. Wait for the fire rescue service to extract them using hydraulic cutting tools and specialized spinal extraction boards.
- The Rare Exceptions (Immediate Threat to Life): You should remove a victim from a vehicle only if staying inside will result in immediate death:
- The engine bay or passenger cabin is on fire or filled with toxic smoke.
- The vehicle is unstable and slipping down a steep embankment or sinking in water.
- The victim is in cardiac arrest, and you must place them on a hard road surface to perform life-saving CPR.
Common Mistakes Bystanders Make at Accident Scenes
When adrenaline runs high, human instinct often drives people to take actions that run completely counter to basic trauma physiology. Avoid these common mistakes:
- Pulling Victims Out Unnecessarily: Forcing someone out of a vehicle or dragging them across asphalt when no immediate environmental threat exists, worsening internal fractures and spinal cord injuries.
- Offering Water or Food: Giving a wounded person a sip of water or a sweet snack can be fatal. If they have internal injuries, water in the stomach can cause immediate vomiting and aspiration into the lungs. Furthermore, if they require emergency surgery upon arrival at the hospital, they must have an empty stomach to safely undergo general anesthesia.
- Ignoring Cervical Spine Precautions: Allowing a dazed victim to sit up, walk around, or tilt their head back to drink fluid, which can damage an un-stabilized neck fracture.
- Delaying the Emergency Call: Spending 10 minutes recording video or taking photos of the wreckage on a smartphone before dialing emergency numbers.
- Crowding the Victims: Surrounding a gasping victim in a tight circle of onlookers, which reduces fresh air flow and significantly increases the victim’s panic and physiological stress.
What NOT to Do During Road Traffic Accidents First Aid
To ensure your actions help rather than harm, memorize these strict limitations on your interventions:
- Do NOT remove a motorcycle helmet: If a motorcyclist has suffered a high-speed crash, their helmet is often acting as a stabilizing splint for a fractured skull or neck. Removing the helmet twists the cervical spine violently. Leave it on unless they are not breathing and you cannot open their airway or perform rescue breaths with the helmet in place.
- Do NOT apply unverified tourniquets: Do not use thin electrical wire, thin string, or narrow shoelaces as a tourniquet. These thin materials fail to stop deep arterial blood flow and instead cut directly through skin and muscle tissue, causing permanent nerve damage. Use a wide cloth strip or a commercial tourniquet.
- Do NOT pull out impaled objects: If a piece of metal, glass shards, or a wooden fragment is impaled deep within the victim’s chest, abdomen, or limbs, leave it right there. The object is currently acting as a plug, sealing off the very blood vessels it has punctured. Pulling it out can cause massive, uncontrollable internal bleeding. Secure it in place with bulky dressings.
Road Traffic Accidents First Aid for Children
A child’s body is anatomically and physiologically distinct from an adult’s. They have softer, more pliable bones, less blood volume, and can lose body heat much faster.
Pediatric Trauma Considerations
- Airway Management: A child’s head is proportionally larger relative to their body. When lying flat on their back, their large occiput (back of the head) naturally flexes the neck forward, which can kink and close their narrow airway. Place a small, folded cloth or hand towel underneath their shoulders to keep their neck in a neutral position.
- Resuscitation Adjustments: For an infant under one year old, check for a pulse on the inside of the upper arm (brachial artery). Perform chest compressions using two fingers in the center of the chest. For a child up to puberty, you can use the heel of just one hand to compress the chest to a depth of about 5 centimeters.
- Emotional Support: Children lack the cognitive capacity to process a major accident. They will often experience severe regression and crying. Speak in a quiet, high-pitched, soothing tone. If possible, keep them within sight of a familiar family member to prevent severe psychological shock.
Road Traffic Accidents First Aid for Elderly Victims
Older adults have a significantly lower physiological reserve, meaning their bodies struggle to cope with the stress of trauma.
Geriatric Trauma Realities
- High Fragility Risk: Due to osteoporosis (weakened bones), elderly individuals can suffer multiple rib fractures or a broken hip from low-speed impacts that would not harm a younger adult. Fractured ribs can puncture the lungs, causing a pneumothorax (collapsed lung).
- Medication Complications: Many older adults regularly take prescription blood thinners (like aspirin, clopidogrel, or warfarin) for heart health. These medications prevent blood from clotting normally, meaning an elderly victim can experience rapid internal bleeding or bleed to death from minor surface lacerations. You must apply direct pressure earlier and for much longer.
- Altered Pain Perception: Due to changes in nerve sensitivity or underlying cognitive health, an elderly person may downplay their injuries, stating they feel “fine” when they are actually suffering from life-threatening internal bleeding. Rely on physical signs like pulse rate and skin appearance rather than just what they tell you.
Essential Items Every Driver Should Carry
The best way to manage a road emergency is to prepare for it long before you turn the ignition key. Every vehicle should be equipped with a functional emergency kit.
The Vehicle Emergency Inventory
| Equipment Category | Specific Item | Primary Lifesaving Purpose |
| Personal Protection | Nitrile Gloves (3 pairs) | Protects the responder from blood-borne pathogens and infections. |
| Hemorrhage Control | Sterile Trauma Gauze Pads & Wide Elastic Roller Bandages | For applying direct pressure and holding pressure dressings over large wounds. |
| Mechanical Tourniquet | CAT or SAM Tourniquet | Instantly stops catastrophic bleeding from severed or crushed limbs. |
| Scene Safety | Reflective Warning Triangle & High-Visibility Vest | Early warning system to prevent oncoming traffic from striking the scene. |
| Rescue Tools | Seatbelt Cutter & Window Glass Breaker Hammer | For cutting jammed seatbelts and shattering tempered side glass for extraction. |
| Thermal Protection | Mylar Space Blanket | Reflects body heat back to prevent hypothermia and combat shock. |
| Illumination | Heavy-Duty LED Flashlight / Headlamp | Essential for managing high-risk scenes and treating victims in low-light or night conditions. |
Legal and Ethical Considerations for Bystanders
A common reason people hesitate to provide First Aid for Accident Victims is the fear of legal liability. Onlookers worry that if they perform CPR or apply a tourniquet and the victim faces complications, they might be sued or harassed by law enforcement.
The Shield of the Good Samaritan Law
- In India: To eliminate this fear, the Supreme Court of India instituted the Good Samaritan Law. Under these strict guidelines, any bystander who steps forward to provide immediate medical or non-medical care to an accident victim is fully protected from any civil or criminal liability.
- Key Protections Provided: You cannot be forced to pay for hospital admission fees, you can choose to remain completely anonymous on police reports, and you cannot be forced to undergo aggressive police questioning or attendance at court trials.
- Global Equivalents: Similar Good Samaritan legislation exists across the United States, Canada, Australia, and many parts of Europe. These statutes protect everyday citizens who step up to provide care in good faith within the scope of their training, ensuring you can act without fear of legal consequences.
Preventing Road Traffic Injuries
While knowing first aid is essential for managing a crisis, the ultimate goal of emergency medicine is prevention. Implementing core safety habits can prevent accidents entirely or significantly reduce the severity of injuries if an impact does occur.
- Consistent Use of Safety Restraints: Always wear a seatbelt, whether you are sitting in the front or the back seat. Seatbelts absorb deceleration forces and prevent your body from slamming into the dashboard or being thrown through the windshield. For motorcyclists, wearing a certified, properly fitted full-face helmet reduces your risk of fatal brain injury by over 40%.
- Rigid Speed Control: Velocity determines the kinetic energy transferred during a collision. Driving within designated speed limits gives you the reaction time needed to brake safely and dramatically reduces the destructive forces during a crash.
- Eliminate Distractions: Operating a vehicle requires your full attention. Avoid using smartphones, texting, adjusting navigation screens, or eating while driving. A split-second distraction at highway speeds can cause your vehicle to travel the length of a football field completely blind.
- Zero Tolerance for Alcohol and Substances: Driving under the influence of alcohol or sedating medications severely impairs your depth perception, slows your reflexes, and clouds your judgment. Never get behind the wheel if you have consumed alcohol.
- Practice Defensive Driving: Always anticipate the unexpected. Maintain a safe following distance from the vehicle ahead of you (the “three-second rule”), watch for pedestrians stepping off curbs, and slow down proactively when approaching blind intersections, school zones, or wet roadways.
Frequently Asked Questions (FAQs)
Should I move an accident victim out of the car?
No, you should almost never move an accident victim from their vehicle. Uncontrolled movement can worsen fractures or sever the spinal cord, leading to permanent paralysis. Leave them in the vehicle unless there is an immediate, life-threatening danger like an active vehicle fire, toxic smoke, or sinking water, or if they require immediate CPR on a flat surface.
What should I do first when arriving at an accident scene?
Your absolute first priority is to ensure scene safety for yourself. Park your vehicle safely away from the crash, activate your hazard lights, and place a reflective warning triangle on the road. Do not approach the damaged vehicles until you are certain you will not be struck by oncoming traffic or exposed to active fires or downed power lines.
How do I stop severe bleeding from an accident wound?
Apply firm, continuous direct pressure over the wound using a clean gauze pad, sanitary pad, or thick cloth. Use the heels of your hands and your upper body weight to press straight down. Hold this pressure uninterrupted for at least 5 to 10 minutes. If bleeding from an arm or leg continues despite direct pressure, apply a mechanical tourniquet 2 to 3 inches above the wound.
Can I give water to an injured person at an accident scene?
No, never give water, food, or oral medication to an accident victim. If the person has internal abdominal injuries, introducing fluids can trigger immediate vomiting, causing them to choke. Furthermore, if they require emergency surgery once they reach the hospital, an empty stomach is necessary to safely administer general anesthesia.
What if the accident victim is unconscious?
If the victim is unconscious, first check if they are breathing normally by looking at their chest for 10 seconds. If they are breathing normally and you do not suspect a spinal injury, place them in the lateral recovery position to keep their airway open. If you suspect a spinal injury, keep them flat on their back and manually hold their head still while checking their breathing closely.
When should CPR be started on an accident victim?
You must start CPR immediately if the victim is completely unresponsive and is either not breathing at all or only making irregular, agonal gasping sounds. Place your hands in the center of their chest and compress firmly at a rate of 100 to 120 compressions per minute, alternating 30 compressions with 2 rescue breaths (or providing continuous, hands-only compressions).
How do I know if someone has a spine injury after a crash?
Assume any victim of a high-speed collision has a spine injury. Strong warning signs include intense neck or back pain, numbness, tingling, or a “pins-and-needles” sensation in the fingers or toes, or an inability to move limbs independently. If the victim is completely unconscious after a major impact, treat them as having a spinal injury.
What should I do if a motorcyclist is wearing a helmet?
Leave the motorcycle helmet on. The helmet acts as a stabilizing splint for a fractured skull or cervical spine. Removing the helmet twists the neck and can cause serious spinal cord damage. The only exception to this rule is if the victim is not breathing and you cannot open their airway or deliver rescue breaths with the helmet in place.
What is the Good Samaritan Law?
The Good Samaritan Law is a legal framework that protects bystanders who provide immediate emergency care to injured victims in good faith. In India and many countries worldwide, this law fully shields you from any civil or criminal liability, meaning you cannot be sued, harassed by police, or forced to pay for hospital fees.
How do I open the airway if I suspect a neck injury?
Use the Jaw-Thrust Maneuver. Kneel behind the victim’s head, place your fingers behind the angles of their lower jawbone, and lift the jaw gently upward and forward. This moves the tongue away from the back of the throat to clear the airway without bending or twisting the neck.
What do I do if an impaled object is sticking out of a wound?
Leave the impaled object exactly where it is. Do not attempt to pull it out or shift it, as the object is currently acting as a plug inside the damaged blood vessels. Removing it can trigger sudden, severe, and uncontrollable internal or external bleeding. Instead, pad around the base of the object with bulky dressings to stabilize it in place.
How can I tell if a victim is going into traumatic shock?
Watch for physical signs of failing circulation. Early indicators include anxiety, restlessness, and a fast heart rate. As shock advances, the victim’s skin will become pale, ash-gray, cold, and soaked in a clammy sweat. Their breathing will become rapid and shallow, and they may show confusion or slurred speech.
How do I handle an open fracture where bone is visible?
Do not try to push the exposed bone back underneath the skin, and do not attempt to straighten the limb. Leave the bone in the position you found it. Loosely drape a clean, damp sterile dressing over the exposed bone and open wound to shield it from debris, then splint the limb to prevent movement.
Quick Emergency Checklist – Road Traffic Accidents First Aid
Save or print this concise emergency reference list. Keep it inside your vehicle’s glove compartment alongside your first aid kit for fast access during a crisis:
- Scene Safety First: Park your vehicle a safe distance away, activate hazard lights, wear a reflective vest, and set up warning triangles 50 to 150 meters ahead of the crash scene.
- Call Emergency Services: Instantly dial 112 (or your local emergency number). Clearly state your exact location, the number of vehicles involved, and any visible hazards.
- Assess Responsiveness: Approach the victim from the front, shake their shoulders gently, and shout loudly to check for a conscious response.
- Control Catastrophic Bleeding: Check for major, spurting wounds immediately. Apply continuous, heavy direct pressure using clean dressings, or deploy a mechanical tourniquet if an extremity is bleeding uncontrollably.
- Open and Protect the Airway: If the victim is unresponsive, use the jaw-thrust maneuver to
- open their airway without bending their neck. Clear away any blood or fluid.
- Check Respiration: Spend 10 seconds looking, listening, and feeling for normal breathing. Treat agonal gasping as non-breathing.
- Perform CPR if Needed: If the victim is not breathing, start chest compressions immediately at a rate of 100 to 120 compressions per minute. Compress to a depth of 5 to 6 centimeters.
- Prevent Traumatic Shock: Lay the victim flat, elevate their legs slightly if injuries permit, wrap them completely in a warm blanket to maintain body heat, and loosen any tight clothing.
- Maintain Spine Immobilization: Keep the head, neck, and torso of conscious or unconscious victims completely still in a neutral position. Do not move them unless they face an immediate threat of fire or explosion.
- Continuous Monitoring & Handover: Stay with the victim, offer quiet reassurance, track their vital signs every 2 minutes, and deliver a structured update to the paramedics when the ambulance arrives.
Conclusion
When a severe road traffic accident occurs, the window of time to preserve human life is incredibly brief. The arrival of an ambulance is the ultimate goal, but the true frontline of survival is formed by everyday citizens who refuse to stand by as passive onlookers. By understanding how to secure a dangerous scene, open a blocked airway, control severe bleeding, and stabilize a fragile spine, you possess the core skills needed to protect a human life during its most vulnerable moment.
Stay calm, follow the structured priorities of trauma care, and act with confidence. Your hands, your voice, and your quick decisions are the bridge that helps an accident victim make it home safely to their family. Take the next step in emergency readiness: locate a certified first aid training center in your community, enroll in a hands-on CPR and trauma care course, and properly equip your vehicle with a high-quality medical kit today.
“This content is for informational and educational purposes only and is not intended as medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any medical decisions.”