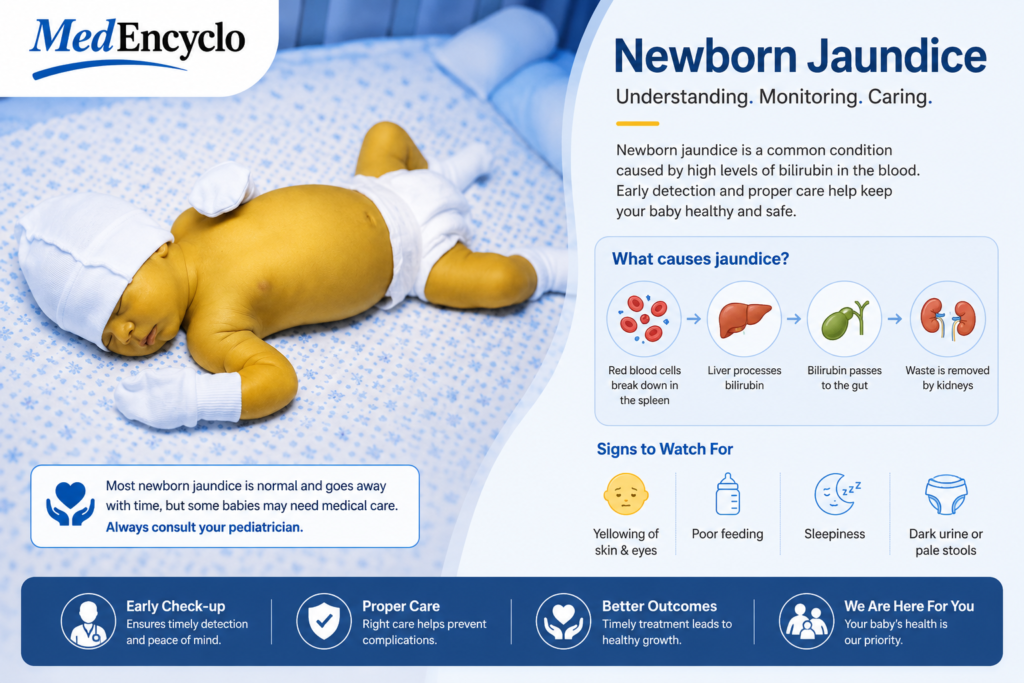
Welcoming a newborn into the world is an incredible journey, but it frequently brings unexpected moments of anxiety. If you have recently noticed a yellowish tint to your baby’s delicate skin or the whites of their eyes, you are definitely not alone.
Neonatal jaundice is one of the most common medical clinical signs seen during the first week of a baby’s life. Many parents notice this subtle change in color and feel an immediate wave of worry.
It is important to understand right from the start: in most newborns, this yellowing is a completely normal, expected temporary phase rather than a sign of a dangerous underlying illness. It is a natural biological transition as your little one adapts to life outside the womb.
What is Neonatal Jaundice?
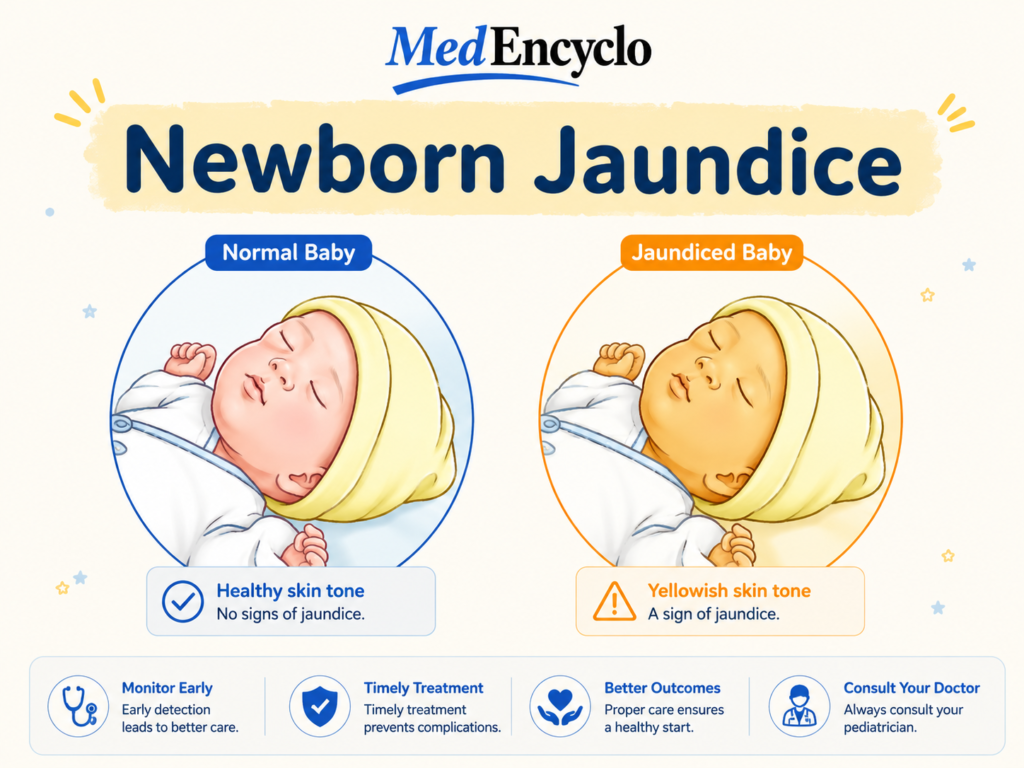
At its core, neonatal jaundice is the visible yellow discoloration of an infant’s skin and the sclera (the white parts of the eyes). This phenomenon occurs due to an accumulation of a naturally occurring yellow pigment called bilirubin in the bloodstream and bodily tissues.
From a clinical perspective, hyperbilirubinemia occurs when total serum bilirubin levels rise above standard physiological thresholds. While this sounds complex, it is helpful to look at it as a simple backlog in your baby’s internal recycling plant.
Why Are Newborns More Prone?
Inside the womb, a fetus requires an extra high concentration of red blood cells to pull enough oxygen from the placenta. The moment your baby takes their first breaths of air, that massive surplus of red blood cells is no longer necessary.
The infant’s body begins breaking down those extra cells rapidly. This normal clearing process produces a large volume of bilirubin all at once. Combined with a tiny, brand-new liver that is still learning how to process this sudden influx, a temporary backup is incredibly common.
The Main Types of Neonatal Jaundice
To provide the best possible Newborn Care, pediatricians categorize this condition into distinct types based on when it appears and what is causing it.
Physiological Jaundice
This is the most common form, affecting up to 60% of full-term infants and up to 80% of preterm babies. It typically appears around the second or third day of life, peaks by day four, and gradually fades away on its own within a week or two as the liver matures.
Pathological Jaundice
Unlike physiological yellowing, pathological jaundice demands immediate attention. It typically appears within the very first 24 hours after birth, shows rapidly escalating bilirubin levels, or persists significantly longer than two weeks. This type points to an underlying medical factor that requires careful investigation.
Breastfeeding Jaundice
This is also known as breastfeeding failure jaundice or sub-optimal intake jaundice. It usually shows up in the first week and occurs when a baby isn’t getting enough breast milk. This may be due to latching difficulties or because the mother’s milk hasn’t fully come in yet. The lack of fluid slows down the baby’s digestive tract, making it harder to eliminate bilirubin through their stool.
Breast Milk Jaundice
This entirely benign type occurs later, usually appearing after the first week of life and potentially lasting for several weeks. It happens in healthy, thriving, breastfed babies. Experts believe certain natural substances in breast milk simply extend the time it takes for the baby’s liver to process bilirubin. It is not a reason to stop breastfeeding.
Causes and Risk Factors
While almost any newborn can experience a mild rise in bilirubin, several distinct risk factors increase the likelihood of needing medical monitoring:
- Prematurity: Babies born before 37 weeks have exceptionally immature livers and sluggish digestive tracts, making Preterm Baby Care vital for tracking jaundice early.
- Blood Type Incompatibility: If a mother has type O blood or Rh-negative blood, and her baby has a different blood type, maternal antibodies can cross the placenta. This causes the baby’s red blood cells to break down much faster than normal (known as ABO or Rh incompatibility).
- Birth Trauma and Bruising: A difficult delivery can sometimes cause significant bruising or a cephalohematoma (a collection of blood under the scalp). As this trapped blood naturally breaks down, it floods the system with extra bilirubin.
- Genetic or Metabolic Factors: Conditions like G6PD deficiency, or structural issues in the biliary system can occasionally block standard elimination routes.
The Pathophysiology Explained Simply
Let’s look at how this happens using a simple analogy. Think of your baby’s bilirubin elimination route as a standard household processing line.
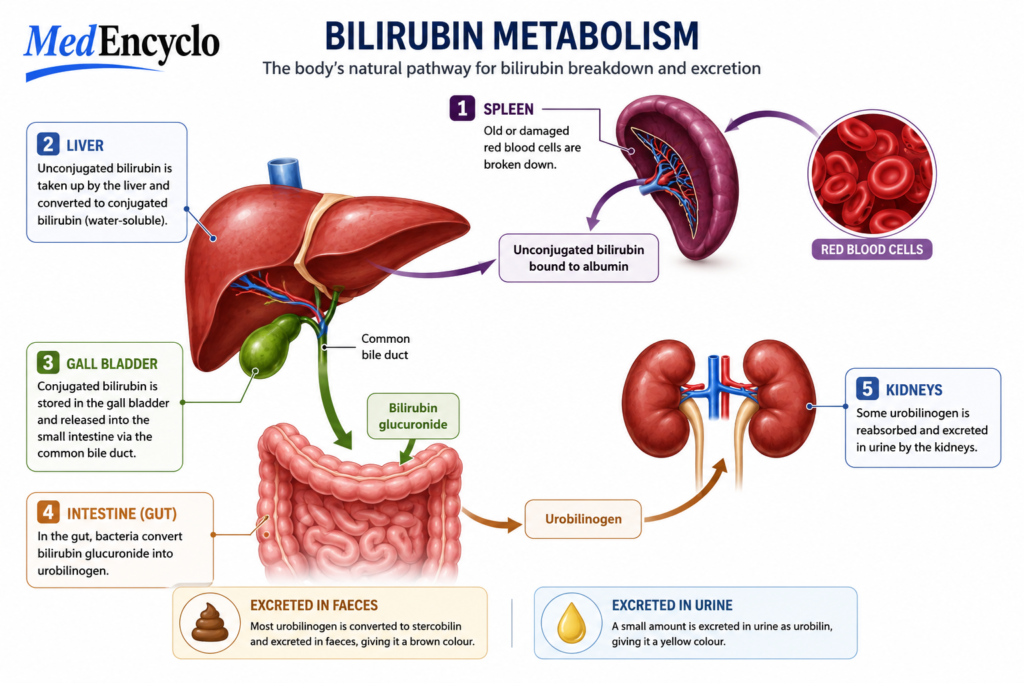
- The Raw Material: Old red blood cells break down, producing “unconjugated” bilirubin. This form is fat-soluble, meaning it dissolves in fat but cannot dissolve in water. It cannot be easily flushed out in urine or stool yet.
- The Processing Center: The bilirubin travels through the bloodstream to the liver. The liver uses enzymes to convert it into “conjugated” bilirubin, which is water-soluble.
- The Delivery Truck: The liver pushes this water-soluble bilirubin into the bile duct, down into the intestines, and safely out of the body in the baby’s diapers.
Because a newborn’s “processing center” is brand new, it runs at a slower speed for the first few days. The unconjugated bilirubin builds up in the bloodstream and settles temporarily under the skin, creating that characteristic yellow look.
Recognizing Signs and Symptoms
The most prominent sign is the yellow color itself. Jaundice typically follows a predictable anatomical path known as Kramer’s progression: it starts on the face and head, then spreads down to the chest, abdomen, legs, and finally the soles of the feet.
To check your baby safely at home, choose a room with plenty of natural daylight. Gently press your finger against your baby’s forehead or nose. If the skin looks pale white for a brief second when you lift your finger, there is likely no jaundice. If the skin looks distinctly yellow, jaundice is present.
In addition to skin changes, parents should observe behavioral cues. A baby with mild jaundice should remain alert, feed vigorously, and wet their diapers regularly. If an infant becomes profoundly sleepy, difficult to wake for feedings, or shows little interest in eating, it could mean bilirubin levels are rising significantly.
How Clinicians Diagnose Jaundice
Pediatric healthcare teams utilize a mix of non-invasive screening and precise laboratory tests to keep babies safe:
- Transcutaneous Bilirubinometry (TcB): This tool uses a handheld device that places a gentle flash of light against your baby’s forehead or chest. It provides an immediate, painless estimate of the bilirubin level through the skin, minimizing the need for needle pokes.
- Total Serum Bilirubin (TSB): If the TcB device shows a high reading, or if the jaundice appears early, we perform a standard heel stick blood test. This gives us an exact measurement of the bilirubin in the blood.
- Additional Workups: If we suspect a blood type incompatibility or an underlying metabolic issue, we will also check the baby’s blood group, perform a Coombs test, or look at a complete blood count (CBC).
Understanding Potential Complications
It is vital to address complications transparently but calmly. When bilirubin levels rise excessively and are left completely untreated, the pigment can cross the blood-brain barrier. This acute condition is known as acute bilirubin encephalopathy.
If this exposure continues over time, it can lead to a rare, permanent form of neurological injury called kernicterus.
⚠️ A Reassuring Note for Parents: Because modern neonatal screening is standard practice globally, kernicterus is exceptionally rare today. Routine checks before hospital discharge ensure that rising trends are caught and treated long before they ever reach dangerous levels.
Medical Management and Modern Treatments
Most infants with mild physiological jaundice require zero treatment; their bodies handle it naturally within a few days. However, when intervention is needed, modern neonatology offers highly safe and effective options.
Phototherapy (Light Therapy)
This is the absolute gold standard for treating neonatal hyperbilirubinemia. The baby is placed under special blue-spectrum medical lamps or on top of a fiber-optic blanket (often called a “biliblanket”) while wearing only a diaper and protective eye patches.
This specific wavelength of blue light passes through the skin and changes the shape of the unconjugated bilirubin molecules through a process called photo-oxidation. It changes the bilirubin into a water-soluble form that the baby’s body can easily flush out in their urine and stool, completely bypassing the liver.
Exchange Transfusion
In rare, critical emergencies where blood type incompatibility causes bilirubin levels to skyrocket dangerously fast, an exchange transfusion is performed in the Neonatal Intensive Care Unit (NICU). This procedure carefully replaces small amounts of the baby’s blood with matching donor blood, rapidly lowering bilirubin levels and removing harmful maternal antibodies.
Home Care and Crucial Parent Guidance
If your baby has mild jaundice and you have been cleared to care for them at home, your absolute best tool is optimized nutrition. Frequent feeding stimulates bowel movements, which helps the baby eliminate bilirubin through their stool.
- Breastfed Infants: Feed your baby every 2 to 3 hours (about 8 to 12 times a day) during the first couple of weeks to maximize milk production and keep their digestive system moving smoothly. Working closely with a specialist can optimize your Breastfeeding technique and ensure good intake.
- Formula-Fed Infants: Offer 1 to 2 ounces of infant formula every 2 to 3 hours.
🚫 Crucial Safety Warning on Sunlight: Older generations often advised putting jaundiced babies in direct sunlight. As modern pediatricians, we strongly advise against this. Direct sunlight carries a high risk of severe sunburn and hypothermia or hyperthermia. Modern medical phototherapy is the only safe way to use light therapy.
Prevention and Proactive Monitoring
While you cannot always prevent neonatal jaundice from developing, you can easily prevent it from becoming a problem:
- Early and Frequent Feedings: Initiating feeding within the very first hours of life sets up a healthy digestive rhythm.
- Universal Screening: Ensure your hospital or birthing center checks your baby’s bilirubin levels using a TcB or TSB test before you pack up to go home.
- Scheduled Follow-ups: Because bilirubin typically peaks between days 3 and 5, your baby should be seen by a pediatrician within 48 hours of leaving the hospital.
Red Flag Signs to Watch For
Please reach out to your pediatrician or visit the nearest emergency medical center immediately if you notice any of these signs:
- The yellow skin color appears within the first 24 hours of life.
- The yellow tint deepens significantly or spreads down past the baby’s abdomen to their knees and feet.
- Your baby becomes intensely lethargic, difficult to wake up, or too sleepy to suck during feedings.
- Your baby develops a high-pitched, unusual cry or arches their back stiffly.
- The jaundice lasts for more than 3 weeks in a full-term infant.
Frequently Asked Questions (FAQs)
Can neonatal jaundice cause permanent harm?
In the vast majority of cases, absolutely not. Mild physiological jaundice resolves completely without leaving any lasting impact. Permanent complications like kernicterus only occur if exceptionally high bilirubin levels are left entirely unmonitored and untreated for an extended period.
Should I stop breastfeeding if my baby is jaundiced?
No, you should not stop breastfeeding. If your baby has breastfeeding jaundice, they simply need to nurse more frequently or require help improving their latch. Even with breast milk jaundice, the condition is completely harmless, and breastfeeding should continue normally. Always speak with your pediatrician before introducing formula supplements.
How long does it typically take for newborn jaundice to go away?
For most full-term infants, physiological jaundice clears up beautifully within 1 to 2 weeks. For babies who are exclusively breastfed or those born slightly early, it can naturally take 3 to 4 weeks to resolve completely.
Why does my jaundiced baby sleep so much?
Bilirubin has a natural, mild sedating effect on the central nervous system. However, if your baby becomes so sleepy that they skip feedings or are very difficult to wake, this is a red flag that requires immediate evaluation by a doctor.
Can a baby get jaundice more than once?
Once physiological jaundice clears up and the baby’s liver reaches full maturity, it does not return. If a baby develops yellow skin later in infancy or childhood, it is caused by completely different medical factors and requires a fresh evaluation.
Conclusion
Finding out your newborn has neonatal jaundice can feel overwhelming during an already exhausting time. However, it is comforting to remember that this is a highly visible, well-understood condition that pediatric teams handle successfully every single day.
By keeping up with early feeding routines, attending your scheduled wellness checkups, and tracking your baby’s behavior, you can navigate this common milestone with confidence. Your baby’s liver will mature in just a few days, their skin will return to its natural tone, and you can focus entirely on enjoying your sweet new addition.
“This content is for informational and educational purposes only and is not intended as medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any medical decisions.”