Introduction
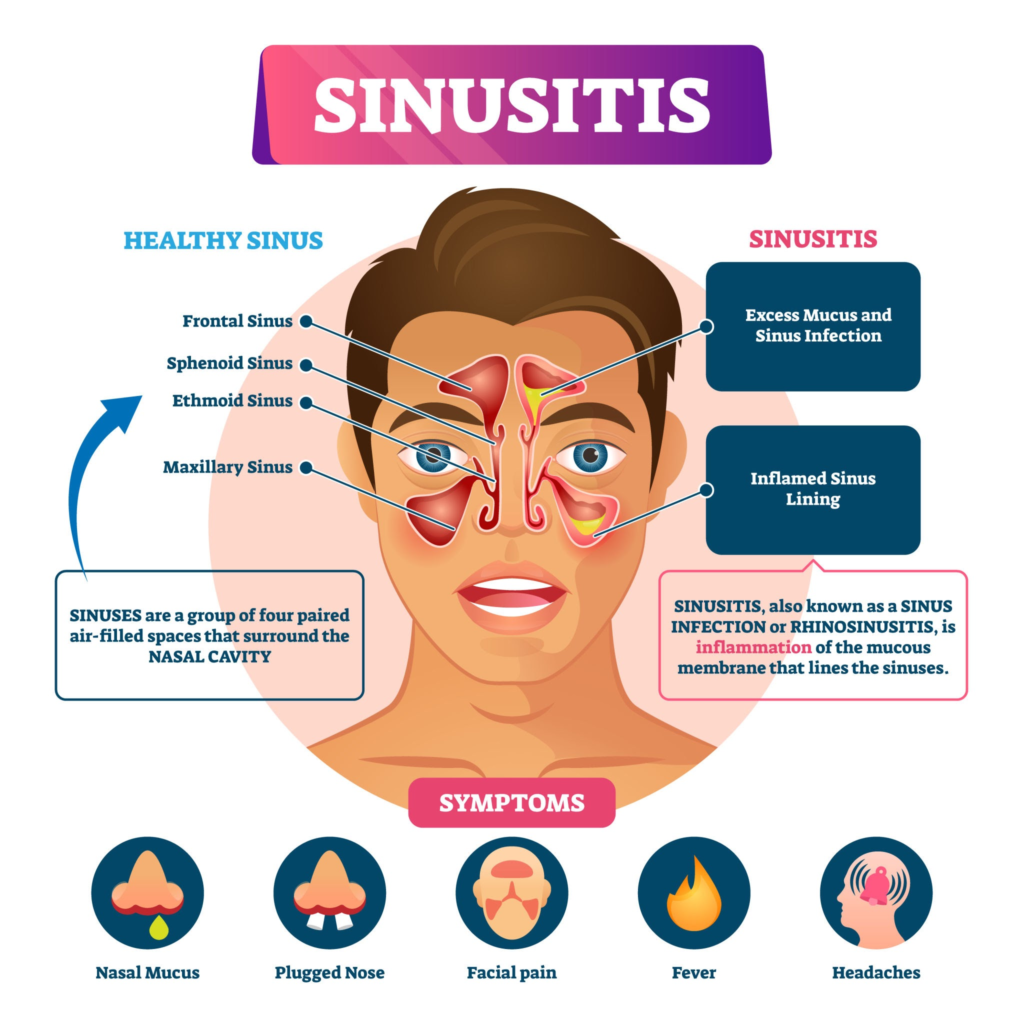
If you have ever felt like your face was carrying an invisible, heavy brick, or if a simple cold turned into weeks of throbbing pressure behind your eyes, you are likely intimately familiar with sinusitis. In plain terms, sinusitis is the swelling or inflammation of the tissue lining the sinuses.
To understand why this happens, it helps to look at the anatomy. Your paranasal sinuses are a connected system of hollow, air-filled cavities hidden behind your forehead, cheekbones, nose, and between your eyes. Their primary job isn’t just to make you miserable when you catch a cold; they actually lighten the weight of your skull, insulate the structures around them, and produce mucus that humidifies the air you breathe while filtering out dust and allergens.
In clinical practice, we see this condition exploded in numbers during seasonal transitions. It is incredibly common worldwide, but it holds a massive footprint in regions with high dust and industrial pollution. For instance, across major urban centers in India, the combination of dense particulate matter (high AQI), soaring pollen counts, and humid microclimates creates a perfect storm. The nasal lining stays in a near-constant state of low-grade irritation, making the transition from a simple “stuffy nose” to a full-blown sinus infection a frequent complaint in our clinics.
Types of Sinusitis
We don’t look at all sinus issues through the same lens. From a medical standpoint, classification is based heavily on duration. When a patient walks into the clinic, establishing the timeline of their symptoms is our first major diagnostic clue.
Recurrent Sinusitis: Some patients experience 4 or more distinct episodes within a single year, with the nasal and sinus mucosa completely returning to normal between each bout. This pattern frequently points toward underlying anatomical issues or environmental triggers that constantly re-open the door to infection.
Acute Sinusitis: This is the classic, sudden onset of symptoms. It usually kicks off as a viral upper respiratory tract infection (a common cold) and lasts less than 4 weeks. Most cases resolve on their own, but if it crosses the 10-day mark without improvement, a secondary bacterial infection might be taking root.
Subacute Sinusitis: A transitional phase where the inflammation persists for 4 to 12 weeks. It represents a stubborn infection or poorly managed allergy that hasn’t quite crossed into permanent tissue changes but is refusing to clear up easily.
Chronic Sinusitis: This is a different beast altogether. If symptoms drag on for more than 12 weeks despite medical intervention, it is classified as chronic. Here, the issue is less about an active, aggressive infection and more about persistent, structural inflammation of the mucosal lining.
Causes & Risk Factors
Sinusitis rarely happens in a vacuum. It is usually the result of an environmental trigger acting on an individual’s underlying anatomy or immune profile.
Infectious Triggers
- Viral Infections: The overwhelming majority of acute sinus infections are viral (such as Rhinovirus, Coronavirus, or Influenza).
- Bacterial Infections: Typically occurs as a secondary infection when trapped mucus becomes a breeding ground. The main bacterial culprits include Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis.
- Fungal Infections: Less common but highly critical, these are typically seen in immunocompromised individuals or patients with allergic fungal sinusitis (AFS), where the body mounts an intense allergic response to environmental molds.
Structural and Environmental Factors
- Allergies (Allergic Rhinitis): Chronic allergic inflammation causes the nasal linings to swell, physically closing off the tiny passages that allow the sinuses to drain.
- Deviated Nasal Septum (DNS): The midline wall dividing your nostrils is rarely perfectly straight. When significantly crooked, it can compress the nasal passages and mechanically block sinus drainage on one side.
- Nasal Polyps: These are soft, noncancerous, teardrop-shaped growths on the lining of your nasal passages or sinuses. They act like literal boulders blocking a stream.
- Pollution, Smoking, and Dust: Regular exposure to cigarette smoke, industrial pollution, and construction dust paralyzes the microscopic hairs (cilia) that line our airways, preventing them from sweeping out mucus.
- Weakened Immunity: Conditions like diabetes, or medications like systemic corticosteroids, lower the body’s natural defenses, making it easier for minor irritations to spiral into deep-seated infections.
Pathophysiology (Explain Simply)
Think of your sinus cavities as a series of small rooms, each connected to a main hallway (the nasal cavity) by a very narrow doorway called an ostium.
Under healthy conditions, the walls of these rooms produce a thin layer of mucus. Microscopic, whip-like structures called cilia act like a coordinated team of sweepers, constantly pushing this mucus out through the narrow doorway into the nose, where it is swallowed or cleared out.
When you catch a cold or encounter a harsh allergen, the lining of these doorways swells shut. Suddenly, the drainage system is completely blocked. The mucus has nowhere to go, so it pools inside the cavity. This stagnant fluid quickly loses oxygen, creating a warm, dark, anaerobic environment that is absolutely ideal for bacteria to colonize and multiply. The resulting pressure buildup against the bony walls of your face is what causes that signature, throbbing sinus pain.
Signs & Symptoms
The clinical picture shifts significantly depending on whether we are dealing with a sharp, acute flare-up or a lingering chronic condition.
| Symptom | Acute Sinusitis | Chronic Sinusitis |
| Facial Pain / Pressure | Sharp, severe, localized over the affected sinus; worsens when bending forward. | Dull, diffuse, generalized facial heaviness; more constant than sharp. |
| Nasal Congestion | Profound, sudden onset; often bilateral. | Persistent, long-term stuffiness; patients adapt to poor nasal breathing. |
| Nasal Discharge | Thick, discolored (yellowish-green) anterior or post-nasal drip. | Frequently clear to thick white/gray, but can turn colored during acute exacerbations. |
| Fever | Common, especially in the first few days of a bacterial flare-up. | Very rare; usually absent unless a new acute infection superimposes. |
| Olfactory Changes | Temporary reduction in smell due to physical blockage. | Long-term hyposmia or anosmia (loss of smell) due to chronic mucosal damage. |
Diagnosis
In the vast majority of acute cases, we do not need expensive imaging or painful procedures. Diagnosis is primarily clinical, built on a thorough history and a physical examination.
During an evaluation, we perform anterior rhinoscopy—using a light and a small speculum to look inside your nostrils. We look for swollen turbinates, septal deviations, and the presence of purulent (pus-like) discharge tracking down from the middle meatus (the drainage area for most sinuses).
When Advanced Tests Are Necessary
- Nasal Endoscopy: Done right in the clinic using a thin, rigid fiber-optic camera. It allows us to look directly into the back of the nasal cavity to see exactly where mucus is trapping or if microscopic polyps are hiding out of plain sight.
- CT Scan of the Paranasal Sinuses (Non-contrast): This is the gold standard for chronic or recurrent cases. Plain X-rays are outdated and largely unhelpful here because they cannot show the fine bony architecture. A CT scan is ordered if a patient is failing medical therapy or if we are planning a surgical intervention. It maps out the exact blockages and anatomical variations.
Complications
The human skull is tightly packed. The sinuses share incredibly thin bony borders with the eye sockets (orbits) and the brain cavity. While complications are rare, they can escalate rapidly if neglected.
- Orbital Cellulitis & Abscess: The ethmoid sinuses sit right between your eyes, separated by a bone as thin as a sheet of paper (the lamina papyracea). Infection can break through this barrier, leading to severe swelling of the eyelid, bulging of the eye (proptosis), pain with eye movement, and potentially permanent blindness if the optic nerve is compressed.
- Intracranial Infections: In exceptionally rare, severe cases, infection can track backward or upward into the brain, causing meningitis (inflammation of the brain linings) or a brain abscess.
- Cavernous Sinus Thrombosis: A life-threatening blood clot at the base of the brain triggered by spreading infection.
- Chronic Lower Airway Irritation: Constant post-nasal drip carrying inflammatory proteins down into the throat can aggravate hyperreactive airways, frequently triggering or worsening asthma attacks.
Management
Managing sinusitis effectively requires a combined strategy: relieving immediate symptoms while correcting the underlying physiological blockages.
A. General Measures
- Aggressive Hydration: Drinking plenty of water thins the consistency of your mucus, making it less sticky and much easier for the cilia to flush out.
- Steam Inhalation: Warm, moist air acts as a natural humectant, soothing irritated nasal membranes and helping to temporarily open up closed nasal passages.
- Rest: Elevating the head with an extra pillow while resting utilizes gravity to help reduce venous engorgement in the nasal lining, making it easier to breathe through the night.
B. Medications (A Clinical Pharmacist’s Perspective)
From a pharmacological standpoint, medication choices must be highly strategic to avoid compounding the patient’s issues.
- Topical Decongestant Sprays (e.g., Oxymetazoline, Xylometazoline): These are powerful alpha-1 adrenergic agonists. They cause rapid vasoconstriction (narrowing of blood vessels) in the nasal lining, providing near-instant relief from congestion.The 5-Day Rule: These must never be used for more than 3 to 5 consecutive days. Overuse causes a downregulation of nasal receptors, leading to severe rebound swelling known as rhinitis medicamentosa. The patient becomes dependent on the spray just to breathe.
- Oral Decongestants (e.g., Pseudoephedrine, Phenylephrine): Systemic alternatives to sprays. They do not cause rebound congestion, but because they cause mild systemic vasoconstriction, they can elevate blood pressure and heart rate. They must be used with caution in patients with hypertension or cardiovascular disease.
- Nasal Corticosteroid Sprays (e.g., Fluticasone, Mometasone): These are the true workhorses for chronic and allergic sinusitis. Unlike systemic steroids, they have minimal absorption into the bloodstream and target the root problem: localized inflammation. They require consistent, daily use for a week or more to reach full efficacy.
- Antihistamines (e.g., Cetirizine, Levocetirizine, Fexofenadine): Highly effective only if the underlying cause is allergic rhinitis. If the sinusitis is purely infectious, first-generation antihistamines can actually backfire by drying out the mucus too much, making it thicker and harder to drain.
- Antibiotics: The general rule in modern medicine is watchful waiting. Over 80% of acute sinusitis cases are viral and will not respond to antibiotics. We reserve antibiotics (typically Amoxicillin-Clavulanate as a first-line option) for cases where symptoms last longer than 10 days without improvement, or if a patient exhibits “double sickening”—getting slightly better from a cold and then suddenly spiking a high fever with severe facial pain.
- Analgesics: Paracetamol (Acetaminophen) or Ibuprofen are essential for managing the inflammatory pain and headache during the acute phase.
C. Surgical Options
Surgery is strictly considered when comprehensive medical therapy has completely failed to provide long-term relief, or when structural barriers prevent drainage.
- Functional Endoscopic Sinus Surgery (FESS): This is a minimally invasive, highly precise procedure performed entirely through the nostrils using endoscopes and micro-instruments. Rather than cutting away tissue indiscriminately, the surgeon carefully widens the natural ostia (doorways) of the sinuses, clears out obstructing polyps, corrects a deviated septum if present, and restores the natural, physiological airflow and drainage pathways.
Home Remedies (Evidence-Informed)
When patients ask about home care, it is vital to separate internet myths from strategies backed by clinical evidence.
- Saline Nasal Irrigation (Neti Pot / Squeeze Bottles): This is highly effective and heavily backed by clinical trials. Flushing the nasal passages with a buffered saline solution physically washes away accumulated crusts, thins thick secretions, and clears out trapped allergens and particulate air pollution.
- The Golden Rule: Always use distilled, sterile, or previously boiled and cooled water. Raw tap water can carry rare but incredibly dangerous pathogens, such as Naegleria fowleri, into the deep nasal vault.
- Warm Compresses: Applying a warm, damp cloth across your cheeks and forehead helps increase local blood flow, relaxes tense facial muscles, and provides a soothing, comforting sensation that eases sinus pressure.
- What Doesn’t Help: Avoiding entire food groups (like dairy) based on the myth that it creates excess mucus. Unless you have a verified allergy to a specific food, dietary restrictions do little to change sinus anatomy or clear a true bacterial infection.
Prevention
Preventing sinus flares is entirely about reducing the workload on your nasal lining and keeping your body’s drainage pathways clear.
- Rigorous Allergy Management: If you know you react to dust mites, pollens, or pet dander, managing those triggers with daily non-sedating antihistamines or nasal steroid sprays during your peak allergy season stops the swelling before it can block your sinus ostia.
- Environmental Protection: In highly polluted or dusty conditions, wearing a well-fitting mask (like an N95 or premium anti-pollution mask) physically protects your nasal mucosa from being bombarded by irritating particles. Using a HEPA air purifier in your bedroom can also dramatically lower the nocturnal inflammatory load.
- Optimize Indoor Humidity: If you live in an exceptionally dry environment or spend all day in a heavily air-conditioned room, using a small cool-mist humidifier keeps your nasal passages from drying out and cracking, preserving the health of your protective mucous barrier.
- Smoking Cessation: Avoiding both firsthand and secondhand tobacco smoke is non-negotiable. Tobacco smoke paralyzes nasal cilia, completely stalling the drainage system.
Red Flag Signs
While most sinus infections are uncomfortable but benign, certain symptoms mean you need to skip the home remedies and head directly to an emergency department or see an ENT specialist immediately.
🚨 Seek Urgent Medical Care If You Experience:
- Periorbital Edema: Any swelling, redness, or visible puffiness around one or both eyes.
- Vision Changes: Double vision (diplopia), blurred vision, or a sudden reduction in your ability to see clearly.
- Ophthalmoplegia: Inability to move your eyeball normally in all directions.
- Severe, Unremitting Headache: A frontal or global headache that is completely unresponsive to standard pain relievers.
- Neurological Shifting: Altered mental status, confusion, a persistently high fever accompanied by a stiff neck (meningismus), or extreme lethargy.
Patient Education Tips
How to Correctly Use a Nasal Spray
Surprisingly, up to 70% of patients use their nasal steroid sprays incorrectly, inadvertently spraying the medication straight onto their nasal septum (the middle wall). This can cause painful crusting, localized bleeding, and won’t help the sinuses.
- Blow your nose gently to clear out major blockages.
- Tilt your head slightly forward, looking down at your toes.
- Hold the spray bottle in your right hand to spray your left nostril.
- Insert the tip slightly into the nostril, pointing it outward toward your left ear, away from the middle wall.
- Press the pump and sniff gently. Do not snort hard, as that sends the medication straight down your throat into your stomach instead of letting it coat the nasal tissues.
- Switch hands: use your left hand to spray your right nostril, pointing toward your right ear.
FAQs (Frequently Asked Questions)
How can I tell the difference between a common cold and a sinus infection?
A cold is typically a viral event that peaks within 3 to 5 days and completely resolves by day 7 to 10. Symptoms like a runny nose gradually improve and the mucus thins out. A bacterial sinus infection persists past 10 days without any sign of structural improvement, or it features “double sickening,” where you feel like you are recovering from a cold but suddenly worsen with intense facial pain and a brand-new fever.
Why won’t my doctor immediately prescribe antibiotics for my sinus pain?
Because antibiotics only kill bacteria; they are completely useless against viruses. Since more than 80-90% of acute sinus flare-ups are viral, taking an antibiotic early won’t speed up your recovery. Instead, it exposes you to unwanted side effects like stomach upset, alters your gut microbiome, and contributes to global antibiotic resistance.
Can I fly if I am currently suffering from a severe sinus infection?
If possible, it is best to avoid flying. Airplanes undergo rapid changes in cabin pressure during takeoff and landing. If your sinus ostia are completely swollen shut, the air trapped inside your sinuses cannot equalize with the cabin pressure. This can cause severe, excruciating pain known as sinus barotrauma, and in rare instances, can cause structural damage to the delicate membranes inside the ear and nose. If you absolutely must fly, using a topical decongestant spray 30 minutes before takeoff and 30 minutes before landing can help keep those pathways open temporarily.
Do lifestyle changes really help chronic sinusitis, or will I eventually need surgery?
Lifestyle changes and structured medical therapy (like daily nasal steroid rinses and allergy optimization) are highly effective and remain our primary line of defense. Surgery is reserved strictly for the minority of patients who have fixed, irreversible anatomical blockages (like large polyps or severe structural deviations) that simply cannot be dissolved or cleared by medications alone.
Can untreated chronic sinusitis affect my lungs or heart?
It does not directly cause heart disease, but it can significantly impact your lower respiratory tract. The constant dripping of inflammatory mucus down the back of the throat (post-nasal drip) frequently irritates the larynx and airways, which can trigger chronic coughing, exacerbate pre-existing asthma, and disrupt your quality of sleep, leading to long-term fatigue.
Conclusion
Dealing with sinusitis can be incredibly exhausting, whether it is a sharp, miserable acute attack or a persistent, low-grade chronic battle that clouds your daily focus. The most critical takeaway is to remember that your sinuses are an intricate drainage system; treatment success relies heavily on patience, consistency, and treating the underlying swelling rather than simply reaching for quick-fix antibiotics or overusing habit-forming decongestant sprays. If your symptoms are stretching past the two-week mark, or if you find yourself clearing your throat and battling facial heaviness multiple times a year, schedule an appointment with a dedicated healthcare professional. A structured, personalized medical plan can comfortably clear those blocked pathways and give you back your quality of life.
“This content is for informational and educational purposes only and is not intended as medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any medical decisions.”