Most of us have experienced that uncomfortable, burning sensation in the chest after an overly indulgent dinner. You might shrug it off as simple indigestion or “acidity.” However, when that burning sensation stops being an occasional post-feast visitor and starts dictating your daily choices, you are likely dealing with something more chronic: Gastroesophageal Reflux Disease (GERD).
In clinical practice, I often see patients who confuse occasional acid reflux with GERD. To clarify the distinction: acid reflux is the physical event where stomach acid backwashes into the food pipe. GERD, on the other hand, is the chronic, structural, or functional progression of this event—typically diagnosed when reflux occurs more than twice a week and begins damaging the esophageal lining or significantly disrupting your quality of life.
Over the last decade, we have observed a steep rise in GERD cases globally, with a particularly dramatic surge in urban areas across India. Modern lifestyles—characterized by high-stress jobs, late-night corporate dinners, sedentary desk routines, and a deep-rooted cultural love for heavy, fried, and heavily spiced foods—have turned acid reflux into one of the most common complaints presenting to gastroenterology clinics today.
Understanding the Mechanism: The Faulty Valve
To understand why GERD happens, it helps to look at the anatomy of your digestive tract. Between your esophagus (food pipe) and your stomach sits a specialized band of circular muscle called the Lower Esophageal Sphincter (LES).
Think of the LES as a sophisticated, one-way pressure valve. When you swallow, this valve relaxes to let food and liquid pass downward into the stomach, and then it tightly clamps shut to protect the delicate tissues of the esophagus from highly acidic gastric juices.
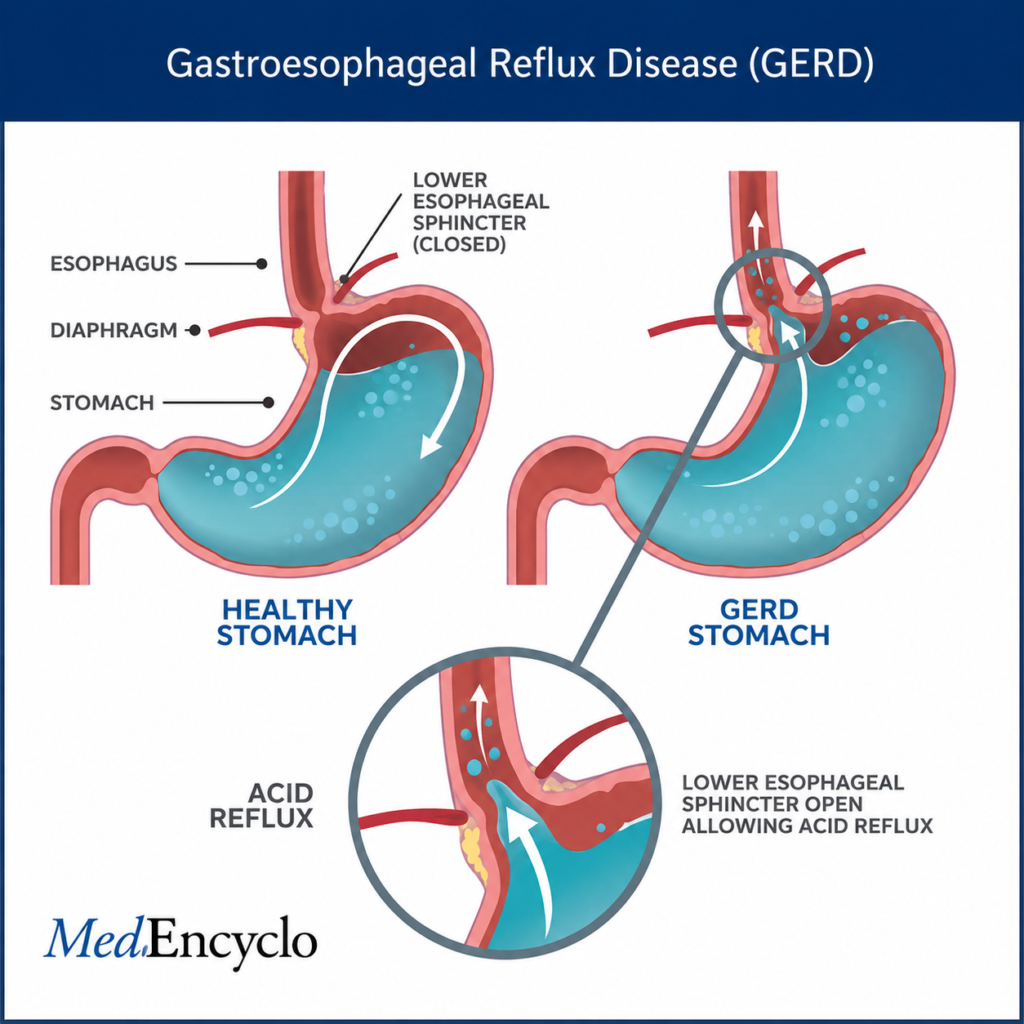
As shown in the diagram above, in a healthy stomach, the closed valve prevents any backflow. In a patient with GERD, this valve becomes abnormally weak or relaxes transiently when it shouldn’t. Because the stomach is inherently built to withstand a highly acidic environment (necessary for breaking down food), it remains unharmed by gastric acid. The esophagus, however, lacks this protective, mucus-rich shield. When the valve fails to close properly, stomach acid escapes upward, irritating and chemically burning the esophageal lining.
Root Causes & Risk Factors
What causes this one-way valve to lose its grip? It is rarely a single factor. In the vast majority of patients, GERD is driven by a combination of anatomical predispositions and daily lifestyle choices:
- Dietary Triggers and Overeating: Consuming large meals stretches the stomach, placing upward mechanical pressure on the LES. Spicy dishes, high-fat fried items, citrus fruits, tomatoes, caffeine, and carbonated beverages all actively lower LES muscle tone or irritate the lining.
- Obesity: Increased abdominal fat exerts continuous physical pressure on the stomach structure, pushing gastric contents upward through the sphincter.
- Smoking and Alcohol Consumption: Nicotine relaxes the LES muscle directly and dries up saliva (which naturally neutralizes mild acid). Alcohol acts as a double blow: it relaxes the sphincter and directly irritates the stomach lining.
- Pregnancy: Hormonal changes (specifically elevated progesterone) relax smooth muscles throughout the body, including the LES. This, combined with the physical pressure of a growing fetus against the stomach, makes acid reflux incredibly common in the second and third trimesters.
- Hiatal Hernia: This occurs when the upper portion of the stomach pushes upward through the small opening in the diaphragm muscle. This structural shift disrupts the natural pressure mechanics of the LES, making reflux almost inevitable.
- Medications: Many patients are surprised to learn their other prescriptions are driving their reflux. Non-Steroidal Anti-Inflammatory Drugs (NSAIDs like ibuprofen or diclofenac), certain blood pressure medications (Calcium Channel Blockers), sedatives, and even some antibiotics can weaken the LES or cause direct mucosal damage.
Signs & Symptoms: Beyond the Burn
While the classic presentation of GERD is highly recognizable, the disease can also manifest in subtle, atypical ways that mimic other medical conditions.
Typical Symptoms
- Heartburn: A burning discomfort or pain that starts behind the breastbone and can radiate upward toward the neck or throat. Many patients notice it intensifies after meals or when lying flat.
- Acid Regurgitation: The bitter, sour-tasting sensation of fluid or undigested food washing back into the mouth or back of the throat.
Atypical and Nocturnal Symptoms
- Chest Discomfort: Can occasionally feel identical to a cardiac event. Clinical Note: Unexplained chest pain must always be evaluated for cardiac causes first before attributing it to GERD.
- Nocturnal Reflux: Symptoms that worsen significantly at night. When flat in bed, you lose the assistance of gravity, allowing acid to pool in the esophagus for hours, frequently waking patients up coughing or choking.
- Extra-esophageal Symptoms: Chronic cough, unexplained hoarseness, a frequent need to clear the throat, or a persistent sore throat. These occur when microscopic droplets of acid reach the vocal cords and respiratory tract, causing chronic irritation (sometimes referred to as Laryngopharyngeal Reflux or LPR).
Types & Clinical Variants
Gastroenterologists look at GERD through specific clinical lenses based on how the tissue responds to the acid exposure:
- Non-Erosive Reflux Disease (NERD): This is actually the most common form, accounting for up to 60-70% of cases. Patients experience severe, classic symptoms of GERD, but when we perform an endoscopy, the esophageal lining looks completely normal and undamaged.
- Erosive Esophagitis: In these cases, the acid has visibly won the battle. Endoscopy reveals clear signs of tissue injury, ranging from mild redness and superficial breaks (erosions) to deep ulcerations in the lower esophagus.
- Barrett’s Esophagus: A serious, long-term cellular adaptation. When exposed to chronic acid assault over many years, the normal squamous cells of the lower esophagus mutate into specialized columnar cells (similar to the lining of the intestines) to protect themselves. This condition requires careful, routine endoscopic surveillance because it acts as a precursor to esophageal adenocarcinoma.
How Gastroesophageal Reflux Disease (GERD)is Diagnosed
In a clear-cut case presenting with classic heartburn and regurgitation, a skilled clinician can often establish a preliminary diagnosis based on history alone. We frequently initiate a short, empiric trial of acid-suppressing medication to see if symptoms resolve.
However, diagnostic testing becomes absolutely necessary if a patient presents with atypical symptoms, shows no improvement with initial medications, or exhibits “red flag” warning signs.
| Diagnostic Tool | What It Entails | When It Is Used |
| Upper Endoscopy (EGD) | A thin, flexible camera tube is guided down the esophagus to visually inspect the lining, check for inflammation, and take small tissue samples (biopsies) if needed. | Recommended for long-standing symptoms, patients over 50, or those presenting with alarming symptoms like difficulty swallowing. |
| 24-Hour Ambulatory pH Monitoring | A tiny sensor probe or wireless capsule measures exact acid levels inside the esophagus over a full day as the patient goes about normal routines. | The gold standard for confirming GERD in complex, non-responsive cases or before planning anti-reflux surgery. |
| Esophageal Manometry | A small catheter measures the rhythmic muscle contractions of your esophagus when you swallow. | Used primarily to rule out primary motility disorders (like achalasia) and to ensure the esophagus pumps well before any surgical intervention. |
Potential Complications of Unchecked Acid
Leaving GERD untreated is not just a matter of enduring daily discomfort; over time, the constant chemical wash can cause permanent structural changes:
- Severe Esophagitis & Ulcers: Deep, painful sores that can bleed, leading to anemia or dark, tarry stools.
- Esophageal Strictures: As chronic ulcers attempt to heal, they lay down dense scar tissue. Over time, this scar tissue contracts, narrowing the interior diameter of the food pipe and making it physically difficult for solid food to pass through.
- Barrett’s Esophagus & Cancer Risk: As highlighted earlier, tissue remodeling can transition into dysplasia, significantly increasing the statistical risk of developing esophageal cancer.
Management: A Three-Tiered Approach
Successfully controlling GERD requires a structured approach that progresses from lifestyle foundations to targeted pharmacology, and in rare cases, structural surgery.
A. Lifestyle Modifications (The Foundation)
Medication can suppress acid production, but lifestyle adjustments fix the underlying mechanical triggers.
- Strategic Meal Timing: This is arguably the most impactful change. Ensure your last meal of the day occurs at least 3 hours before you lie down in bed. Going to sleep with an actively churning, full stomach invites nocturnal reflux.
- Gravity Assists: Elevate the head of your bed by 6 to 8 inches. Using extra pillows simply bends your neck and increases abdominal pressure; instead, use physical bed risers or a firm wedge pillow to slope your entire upper torso upward.
- Conscious Weight Management: Losing even 5-10% of body weight can markedly reduce intra-abdominal pressure, giving the LES immediate mechanical relief.
- Tailoring Your Plate: Avoid known trigger foods. In the context of rich culinary traditions like those in India, this often means limiting deep-fried evening appetizers (like samosas and pakoras), reducing heavy fats (ghee, butter), minimizing strong spices late in the day, and capping excessive intake of strong milk tea (chai) or coffee, which heavily relaxes the LES.
B. Medications (The Pharmacist’s Insight)
As a clinical pharmacist, I cannot emphasize enough that these choices should be strategic, not random over-the-counter habituation.
[Antacids] --> Fast, temporary relief (Neutralize existing acid)
[H2 Blockers] --> Moderate, longer relief (Block histamine-2 signals)
[PPIs] --> Deep, systemic suppression (Shut down chemical acid pumps)- Antacids & Alginates: Over-the-counter liquids or chewable tablets containing magnesium, aluminum, or calcium carbonate provide immediate, temporary relief by neutralizing the acid already sitting in your stomach. Alginate-containing formulas form a physical foam barrier that floats on top of the gastric contents, mechanically blocking acid from entering the esophagus.
- H2 Receptor Antagonists (H2RA): Medications such as famotidine or chemical alternatives reduce acid production by blocking histamine signals to parietal cells. They take longer to kick in than antacids but provide relief for several hours.
- Proton Pump Inhibitors (PPIs): Drugs like omeprazole, pantoprazole, rabeprazole, and esomeprazole are the cornerstones of medical therapy. They bind directly to the acid-producing pumps inside your stomach cells, shutting down acid production at the source. They allow damaged esophageal tissue to heal efficiently.
- Prokinetics: Medications like domperidone or itopride are occasionally co-prescribed to stimulate faster stomach emptying, ensuring food moves into the intestines quicker so it cannot backwash.
C. Surgical Options
When lifestyle changes and optimal medication routines fail to provide relief, or if a patient simply wants to avoid taking medications for the rest of their life, surgery is considered.
The standard intervention is a Laparoscopic Nissen Fundoplication. In this minimally invasive procedure, a surgeon takes the very top portion of the stomach (the fundus) and wraps it securely around the lower esophagus. This effectively reinforces and recreates a tight, functional physical valve to stop reflux mechanically.
Home Remedies: Fact vs. Fiction
Many patients try home remedies before seeking medical advice. It is vital to separate what actively helps from what can actually worsen the condition.
What Works:
- Sipping Warm Water: Helps clear residual acid from the esophagus and gently stimulates downward peristalsis (digestive movement).
- Chewing Sugar-Free Gum: Stimulates saliva production. Saliva contains natural bicarbonate, which acts as a mild, continuous, natural buffer against acid.
- Smaller, Fragmented Meals: Eating five small meals instead of three large, dense plates prevents stomach over-distension.
What Backfires (The Myths):
- Drinking Direct Citrus or Apple Cider Vinegar: While some internet blogs claim vinegar corrects stomach pH, placing highly acidic liquids into an already inflamed, raw food pipe frequently causes direct mucosal pain and worsens esophagitis.
- Drinking Full-Fat Cold Milk: While cold milk feels soothing for the first two minutes, the high fat and calcium content triggers a “rebound effect,” signaling the stomach to produce even higher volumes of acid shortly afterward.
Long-Term Prevention Strategies
Preventing the recurrence of GERD relies on sustainable, long-term habits rather than short-term restrictions.
- Avoid tight-fitting clothing or belts that constrict the waistline, which mechanically forces acid upward.
- Incorporate stress-reduction practices (like yoga or mindful breathing techniques); physical stress alters gut motility and lowers your threshold for pain perception, making normal amounts of acid feel significantly more painful.
- Adopt a post-dinner habit of taking a gentle 15-minute walk rather than moving directly from the dining table to the couch.
Red Flag Signs: When to See a Doctor Immediately
While GERD is manageable, certain symptoms indicate a medical emergency or advanced structural damage. If you or a loved one experience any of the following, do not wait for lifestyle modifications to work—seek professional medical evaluation immediately:
- Dysphagia: A physical feeling that food is getting stuck or lodged in your throat or chest while swallowing.
- Odinophagia: Sharp pain experienced specifically when swallowing food or liquids.
- Unexplained Weight Loss: Dropping weight without a change in diet or exercise, which can point to underlying malignancies.
- Hematemesis or Melena: Vomiting blood (which may look like dark coffee grounds) or passing black, foul-smelling, tarry stools—both indicate active upper gastrointestinal bleeding.
- Persistent Unresponsiveness: Severe symptoms that fail to show any improvement even after a consistent 2-to-3-week course of daily PPI therapy.
Patient Education: The Pharmacist’s Corner on PPI Misuse
In clinical practice, I regularly encounter patients who take their PPI medications incorrectly, leading them to believe the treatment is ineffective.
- Timing is Key: PPIs (like pantoprazole or omeprazole) must be taken 30 to 60 minutes before your first meal of the day. They require the stomach’s acid pumps to be resting but primed for activation to bind to them successfully. Taking a PPI after breakfast or right before bed reduces its therapeutic efficacy significantly.
- Avoid the “On-Demand” Trap: Unlike antacids, PPIs do not work instantly. They take several days of consecutive use to achieve full acid suppression. Taking them only on days you feel heartburn is a pharmacologically ineffective strategy.
- The Danger of Chronic Self-Medication: Over-the-counter availability has led to widespread chronic use of PPIs for years without doctor supervision. Long-term, unmonitored acid suppression can reduce the absorption of essential nutrients (like Vitamin B12, calcium, and magnesium) and alter gut flora, increasing susceptibility to infections like Clostridium difficile. Use them diligently for the duration prescribed by your doctor, and focus on tapering off under medical guidance once the tissue has healed.
Frequently Asked Questions (FAQs)
Can GERD cause breathing difficulties or asthma?
Yes. Microscopic amounts of acid can escape the esophagus and spill into the respiratory tract, causing irritation or spasms in the airways. This can trigger a chronic dry cough, wheezing, or worsen pre-existing asthma symptoms.
Is it safe to take acid blockers everyday for years?
While generally safe under medical supervision for severe conditions (like severe Barrett’s esophagus), long-term use should be carefully monitored. Prolonged use can lead to poor absorption of bone calcium and vitamin B12. The goal should always be to use the lowest effective dose for the shortest period required.
Why does my acid reflux feel worse when I sleep on my right side?
Anatomically, the stomach curves to the left side of your body. When you sleep on your left side, the junction between your esophagus and stomach stays elevated above the level of gastric acid. Sleeping on your right side places that junction beneath the acid pool, making it easier for fluid to leak through the LES.
Can anxiety cause or worsen GERD?
Anxiety doesn’t necessarily cause more acid to be produced, but it drastically increases your body’s nerve sensitivity (visceral hypersensitivity). This means even tiny, normal amounts of reflux feel intensely painful. Furthermore, stress slows down overall digestion, leaving food in the stomach longer.
I have a chronic cough but no heartburn. Could it still be GERD?
Absolutely. This is often referred to as “silent reflux” or Laryngopharyngeal Reflux (LPR). The acid travels all the way up into the throat without lingering long enough in the lower esophagus to cause classic heartburn pain, presenting primarily as a throat irritation or chronic cough.
Conclusion
GERD can feel exhausting, but it is highly treatable. By combining structured lifestyle changes—like earlier dinners and smarter food choices—with accurate, short-term medical therapy, the vast majority of patients achieve complete symptom control and successfully protect their digestive health. Listen to your body, avoid the trap of unmonitored self-medication, and work closely with your healthcare team to build a sustainable path to relief.
“This content is for informational and educational purposes only and is not intended as medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any medical decisions.”