Introduction
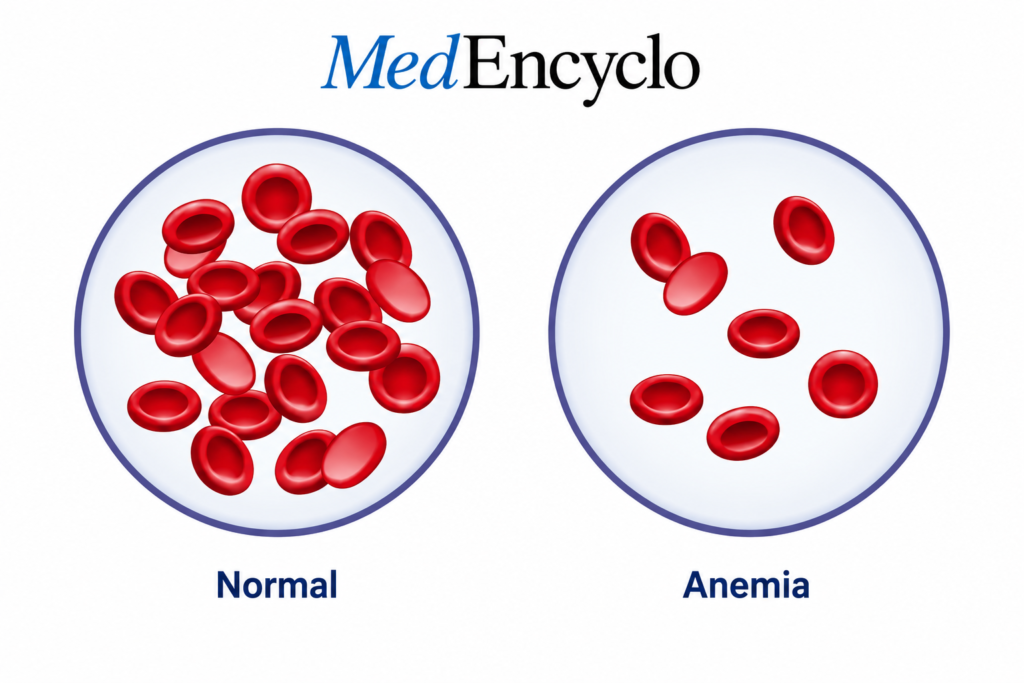
Anemia is one of the most widespread clinical conditions encountered in global healthcare, yet it remains profoundly underdiagnosed. At its core, the condition arises when your blood has a lower-than-normal concentration of healthy red blood cells or hemoglobin.
In everyday practice, I see this manifested as chronic, unexplained exhaustion that a good night’s sleep simply cannot fix. According to data from the World Health Organization (WHO), it affects nearly 2 billion people globally.
The prevalence is particularly stark in developing regions like India. Here, a combination of dietary habits, structural healthcare gaps, and physiological demands means that over 50% of pregnant women and young children actively live with reduced hemoglobin levels. This makes it a major public health priority alongside managing other chronic metabolic challenges like diabetes.
What is Anemia?
To understand this condition, it helps to view your blood as a highly specialized delivery logistics system. Your red blood cells (RBCs) act as cargo trucks. Inside these trucks sits a specialized protein called hemoglobin, which acts as the actual binding dock for oxygen molecules.
When you breathe in, oxygen binds to hemoglobin in the lungs. The heart then pumps these cells throughout the body to drop oxygen off at your brain, muscles, and organs.
If you develop a drop in hemoglobin, your body’s tissues are basicially starved of oxygen. Your heart has to work twice as hard to pump a lower volume of oxygenated blood, leading directly to the classic presentation of clinical fatigue.
The Core Types: Iron vs. Vitamin B12 Deficiency
While there are dozens of reasons why a person’s RBC count might drop—ranging from genetic mutations to complications of chronic kidney disease—two specific nutritional deficiencies account for the vast majority of outpatient cases.
1. Iron Deficiency Anemia (IDA)
This is the single most common variant worldwide. Iron is the primary chemical backbone needed to manufacture hemoglobin. Without adequate iron, your bone marrow simply cannot build the core protein structure required to carry oxygen. The resulting cells are typically small (microcytic) and pale (hypochromic).
2. Vitamin B12 Deficiency Anemia
Also known as macrocytic or megaloblastic anemia, this occurs when the body lacks vitamin B12 (cobalamin). B12 is essential for cellular DNA synthesis. Without it, the developing red blood cells in your bone marrow cannot divide properly. They grow abnormally large (macrocytic) and structurally fragile, often dying before they can even enter circulation.
Other Notable Types
- Folate Deficiency: Similar to B12 deficiency, it causes large, abnormal cells due to poor DNA synthesis.
- Hemolytic Varieties: Conditions where the body prematurely destroys its own red blood cells before their natural 120-day lifespan ends.
- Aplastic Varieties: A rare, severe bone marrow failure condition where the body stops producing enough new blood cells entirely.
Primary Causes & Risk Factors
Anemic presentations rarely happen without a clear trigger. Determining why the deficiency exists is the most crucial part of a medical evaluation.
A. Iron Deficiency Triggers
- Chronic Blood Loss: In adult women, heavy menstrual bleeding (menorrhagia) is the top culprit. In older adults, occult gastrointestinal bleeding from ulcers or polyps must be ruled out.
- Elevated Physiological Demand: Pregnancy and rapid childhood growth spurts spike the body’s baseline requirement for iron.
- Dietary Gaps: Diets chronically low in highly bioavailable iron sources quickly deplete the body’s structural reserves.
B. Vitamin B12 Deficiency Triggers
- Strict Plant-Based Diets: Vitamin B12 is synthesized exclusively by microorganisms and is found naturally only in animal-sourced products.
- Malabsorption Syndromes: Conditions like Celiac disease, Crohn’s disease, or a history of gastric bypass surgery impair the gut’s ability to absorb nutrients.
- Medication Interference: Many patients don’t realize that long-term use of common medications—such as metformin for blood sugar regulation or proton pump inhibitors (PPIs) for acid reflux—can severely reduce B12 absorption.
The Pathophysiology Made Simple
Let’s use a construction analogy to visualize how these deficiencies damage your health. Think of your bone marrow as a busy factory building delivery houses (red blood cells).
[Iron Supply] --------> Hemoglobin Production -------> Stable, Normal RBCs
[Vitamin B12] --------> Cellular DNA Blueprint -------> Correct Cell DivisionIf the factory runs out of iron, it lacks the raw bricks needed to assemble the internal machinery. It resorts to building tiny, weak, half-empty houses that cannot hold enough oxygen.
If the factory runs out of Vitamin B12, it loses the master blueprint for construction. The building process stalls, cell division fails, and the factory releases giant, misshapen, structurally unsound houses that break down almost immediately. Furthermore, B12 is vital for maintaining the protective insulation (myelin) around your nerves, which is why a B12 shortfall causes neurological symptoms that iron deficiency does not.
Signs & Symptoms to Watch For
The signs of a drop in hemoglobin can sneak up on you gradually. Your body adapts to the slow decline in oxygen over months, meaning you might not notice a problem until your levels drop significantly.
General Symptoms
- Profound Fatigue & Lethargy: A persistent lack of physical energy.
- Exertional Dyspnea: Getting unusually winded just walking up a single flight of stairs.
- Postural Dizziness: Lightheadedness when standing up quickly.
- Pallor: Visible paleness in the skin, fingernails, and the inner lining of the lower eyelids (conjunctival pallor).
Vitamin B12-Specific Features
Because B12 is essential for neurological preservation, unique symptoms can emerge alongside general weakness:
- Peripheral Neuropathy: Symmetrical tingling, numbness, or a “pins and needles” sensation in the hands and feet.
- Glossitis: A smooth, swollen, unusually red, and painful tongue surface.
- Cognitive Decline: Mild memory lapses, brain fog, irritability, or balance disturbances.
The Clinical Diagnostic Pathway
You cannot accurately diagnose this condition based on symptoms alone. A definitive treatment plan requires precise laboratory confirmation via targeted blood panels.
| Laboratory Evaluation | What It Measures | Clinical Interpretation |
| Complete Blood Count (CBC) | Hemoglobin (Hb) & Hematocrit | Confirms the presence and severity of the systemic drop. |
| Mean Corpuscular Volume (MCV) | The physical size of the RBCs | Low MCV indicates microcytic (Iron); High MCV indicates macrocytic (B12/Folate). |
| Serum Ferritin | The body’s deep cellular iron reserves | The most accurate marker for evaluating true iron storage depletion. |
| Serum B12 & Folate Levels | Active circulating vitamin levels | Directly identifies cobalamin or folic acid shortfalls. |
| Peripheral Blood Smear | Visual microscopic shape evaluation | Confirms abnormal shapes, like hypersegmented neutrophils in B12 deficiency. |
Potential Health Complications
Leaving an underlying deficiency unchecked can cause progressive, widespread damage across multiple organ systems.
- Cardiovascular Strain: Chronic oxygen deprivation forces your heart to beat faster and pump harder. Over time, this persistent volume overload can cause cardiomegaly (heart enlargement) or precipitate high-output heart failure.
- Adverse Pregnancy Outcomes: Severe maternal iron deficiency increases the statistical risk of premature births, low infant birth weight, and postpartum depression.
- Irreversible Neurological Damage: If a Vitamin B12 deficiency is neglected for years, the degradation of the spinal cord’s myelin sheath can progress from basic tingling to permanent nerve damage, balance loss, and cognitive decline.
Evidence-Based Management Strategies
Correcting a deficiency requires a multi-pronged approach that combines targeted dietary changes with clinical medical interventions.
A. Dietary Adaptations (With an Indian Context)
Adjusting what you eat is an important first step, but it must be tailored to your specific lifestyle and dietary restrictions.
For Iron Enhancement: Incorporate dark green leafy vegetables (spinach, amaranth), legumes, lentils, and unrefined sweeteners like jaggery. For non-vegetarians, lean meats and liver provide highly absorbable heme iron.
For Vitamin B12 Enhancement: Vegetarians should prioritize dairy products like milk, curd, paneer, and fortified cereals. Non-vegetarians can easily obtain B12 through eggs, fish, and poultry.
B. Pharmacological Supplementation
Dietary changes alone are often insufficient to rebuild deeply depleted corporate stores, necessitating clinical supplementation.
- Iron Therapies: Oral ferrous salts (like ferrous sulfate or ascorbate) are standard. For patients with severe malabsorption or intolerance, modern intravenous iron infusions offer rapid, safe replenishment.
- Vitamin B12 Therapies: If caused by dietary choices, oral methylcobalamin tablets work well. If caused by an absorption failure (such as pernicious anemia), lifelong intramuscular injections (cyanocobalamin) are required to bypass the dysfunctional gut completely.
C. Addressing the Root Cause
Treating the blood count is a temporary fix if the underlying leak is ignored. Clinical teams must investigate and address the structural cause, whether that means treating a bleeding gastric ulcer, managing underlying malnutrition, or adjusting a medication regimen.
Proactive Prevention
The easiest way to manage a nutritional deficiency is to prevent it from developing in the first place.
- Consume a Balanced Diet: Ensure your meals combine diverse protein sources, complex carbohydrates, and micro-nutrient-dense vegetables.
- Routine Screening Regimens: High-risk groups—including menstruating individuals, pregnant women, and strict vegans—should request a routine CBC and ferritin panel during annual health checkups to catch dropping levels early.
Clinical Red Flags
While mild deficiencies can be managed routinely, certain symptoms warrant immediate medical evaluation at an emergency department:
Acute Chest Pain or Palpitations: Indicating severe cardiac hypoxia (oxygen starvation).
- Sudden, Severe Shortness of Breath: Even while resting completely still.
- Progressive Neurological Deficits: Rapidly worsening loss of balance, difficulty walking, or sudden confusion.
Critical Patient Education Tips
One common mistake people make is taking their supplements incorrectly, which can completely compromise their recovery.
- Optimize Your Iron Intake: For maximum absorption, take your iron tablet on an empty stomach with a source of Vitamin C (like a glass of fresh lemon water).
- Avoid Calcium Interferences: Never take your iron supplement with milk, calcium tablets, antacids, tea, or coffee. The polyphenols and calcium ions bind tightly to iron in the gut, rendering it completely unabsorbable.
- Commit to the Full Course: Many patients stop taking their iron pills as soon as their energy returns and their hemoglobin stabilizes. However, it takes an additional 3 to 6 months of continuous therapy after hemoglobin normalizes to fully restore your body’s deep tissue ferritin reserves.
Frequently Asked Questions
Can I have anemia even if my skin doesn’t look pale?
Yes. Paleness is a subjective sign that often doesn’t appear until hemoglobin levels drop significantly. Many individuals with mild to moderate deficiencies maintain normal skin tone but still experience severe internal fatigue and reduced exercise tolerance.
Why do iron tablets make my stool turn black?
This is a completely normal, harmless side effect. Your gut only absorbs a fraction of the oral iron dose; the unabsorbed iron compounds pass through your digestive tract, turning your stool a dark green or black color. It is not a sign of internal bleeding.
Can I cure a Vitamin B12 deficiency simply by eating more spinach?
No. Vitamin B12 is entirely absent from plant-based foods like spinach, kale, and fruits. Plant sources can provide folate and iron, but true B12 must come from animal products, fortified foods, or direct medical supplements.
How long does it take to feel better once treatment starts?
Most patients notice a significant improvement in their energy levels within 2 to 3 weeks of starting appropriate, consistent supplementation. However, your laboratory parameters will take several months to completely normalize.
Is it safe to take iron supplements without a blood test?
No. Taking high doses of iron without a confirmed deficiency can lead to iron overload (hemochromatosis). Excess iron deposits can accumulate in and damage your liver, heart, and pancreas, so always confirm your levels with a blood test first.
Conclusion
Anemia is a highly treatable condition, but it requires an accurate diagnosis and a commitment to targeted therapy. By understanding whether your body is short on iron or Vitamin B12, optimizing how you take your supplements, and addressing the root cause, you can successfully reclaim your energy, focus, and overall vitality. If you have been living with persistent, unexplained fatigue, speak with your healthcare provider to schedule a routine blood panel.
“This content is for informational and educational purposes only and is not intended as medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any medical decisions.”