Tuberculosis, commonly known as TB, is an ancient infectious disease that continues to challenge modern medicine. Despite being entirely preventable and curable, it remains one of the leading infectious killers globally.
In clinical practice, we encounter a widespread misconception that this condition is a shadow of the past. However, for anyone living or working in regions with high case volumes, it is an everyday reality.
India bears a disproportionately high burden of global cases, accounting for more than a quarter of the world’s total infections. This reality highlights the urgent need for community awareness, early screening, and strict adherence to modern treatment guidelines.
When a patient enters a clinic with a persistent cough, it is crucial to look beyond standard respiratory infections. Understanding how this pathogen behaves, how it spreads, and how our bodies defend against it can demystify the diagnosis and empower patients to complete their recovery safely.
What is Tuberculosis?
Tuberculosis is a chronic bacterial infection caused by a specific, slow-growing pathogen known as Mycobacterium tuberculosis. Unlike common viral infections or rapid bacterial bronchitis, this micro-organism possesses a unique, waxy cell wall rich in mycolic acid.
This distinctive structural feature shields the bacterium from standard antibiotics and enables it to survive inside human host defenses for prolonged periods.
Transmission of the infection occurs almost exclusively through the air. When an individual with active disease in their lungs coughs, sneezes, speaks, or sings, they release microscopic droplet nuclei into the surrounding air.
These tiny droplets can remain suspended in poorly ventilated spaces for several hours. If a nearby individual inhales these particle nuclei, the bacteria can bypass the upper respiratory defenses and settle deep into the tiny air sacs of the lungs.
One important thing people often overlook is that you cannot catch this infection from casual surface contact. Sharing utensils, shaking hands, or touching clothing or bedding used by a patient does not transmit the bacteria.
Prolonged, close contact in enclosed spaces with an untreated, infectious individual is the primary driver of transmission.
Types of Tuberculosis
To properly manage this condition, we must differentiate between its various clinical presentations. It is not a uniform illness; its behavior depends entirely on the location of the infection and the strength of the patient’s immune response.
Pulmonary vs. Extrapulmonary TB
The disease is broadly categorized by the organ systems it affects:
- Pulmonary TB: This is the most common form, accounting for approximately 80% of all clinical cases. The bacteria primarily target the lungs, where oxygen levels are high, creating an ideal environment for them to replicate. This form is highly contagious when active.
- Extrapulmonary TB: In many patients, the infection spreads beyond the respiratory system via the bloodstream or lymphatic network. It can establish itself in almost any organ, including the lymph nodes, spine, brain, kidneys, gastrointestinal tract, or joints. Extrapulmonary presentations are generally non-contagious unless they involve open wounds or surgical procedures.
Latent TB vs. Active TB
Another vital distinction lies between a quiet, contained infection and an active, symptomatic state. The table below outlines the core differences between these two phases:
| Clinical Feature | Latent TB Infection (LTBI) | Active TB Disease |
| Symptoms | None. The patient feels completely healthy. | Present (Cough, fever, weight loss, night sweats). |
| Contagiousness | Cannot spread the bacteria to others. | Highly contagious if the infection is pulmonary. |
| Test Results | Positive skin or blood test; normal chest X-ray. | Positive sputum culture, molecular test, or abnormal X-ray. |
| Bacterial State | Bacteria are alive but dormant and contained. | Bacteria are actively multiplying and destroying tissue. |
| Medical Action | Preventive therapy to avoid future activation. | Immediate multi-drug regimen to cure the disease. |
Causes & Risk Factors
While inhalation of the bacterium is the definitive cause of the infection, not everyone exposed will fall ill. The transition from exposure to active disease depends heavily on specific environmental and biological vulnerabilities.
Environmental Factors
Overcrowding and poor ventilation are primary drivers of transmission. Enclosed, poorly lit spaces allow droplet nuclei to accumulate in the air, increasing the likelihood of inhalation.
In clinical practice, we frequently observe clusters of cases in densely populated urban housing, correctional facilities, and long-term care institutions.
Systemic Immunosuppression
A robust immune system can usually contain the bacteria indefinitely. However, when systemic defenses weaken, the risk of developing active disease rises significantly.
- HIV/AIDS: This remains the most potent risk factor for progression. The destruction of T-lymphocytes deprives the body of the exact immune cells needed to contain the bacteria.
- Diabetes Mellitus: Uncontrolled blood sugar impairs the function of white blood cells, making diabetic patients three times more likely to develop active disease.
- Immunosuppressive Therapies: Long-term corticosteroid use, chemotherapy, and biologic therapies for autoimmune conditions (such as TNF-alpha inhibitors) significantly lower protective barriers.
Lifestyle and Nutritional Status
Severe malnutrition weakens cell-mediated immunity, stripping the body of its structural defenses. Additionally, chronic tobacco smoking alters the mucosal lining of the respiratory tract and impairs the clearing mechanism of the bronchial cilia. This structural damage makes it much easier for inhaled bacilli to anchor themselves deep in the lungs.
Pathophysiology: What Happens inside the Lungs
To understand why this infection requires months of specialized therapy, we must look at how it interacts with our immune cells.
When the bacteria reach the microscopic air sacs (alveoli), specialized immune cells called alveolar macrophages quickly engulf them. In a standard bacterial infection, these macrophages would easily digest and eliminate the invader.
However, the specialized waxy outer coating of Mycobacterium tuberculosis prevents this destruction. Instead of dying, the bacteria begin to multiply safely inside the very immune cells sent to kill them.
[Inhaled Bacilli] ──> [Engulfed by Macrophages] ──> [Bacteria Resist Destruction]
│
[Granuloma Formed (Containment)] <── [Immune Cells Wall Off Infection] <───┘Realizing the localized threat, the body deploys a broader immune response, sending T-lymphocytes and other white blood cells to surround the infected macrophages. These cells tightly cluster together to form a microscopic structure called a granuloma.
Think of a granuloma as a biological containment wall. The immune system cannot always kill the bacteria outright, so it builds a cellular prison around them to keep them from escaping.
Inside this wall, the tissue undergoes a form of cell death known as caseous necrosis, creating a soft, cheese-like material at the center of the structure.
If the immune system remains strong, the bacteria stay locked behind this wall indefinitely, resulting in latent infection. However, if the body’s defenses falter years later, this protective wall breaks down. The cheese-like center liquefies, the granuloma ruptures, and thousands of active bacteria spill into the airways, causing active disease.
Signs & Symptoms to Watch For
The clinical presentation of active pulmonary disease develops slowly, often creeping up over weeks or months. Because the early signs mimic general fatigue or a lingering cold, many individuals delay seeking medical attention.
A persistent cough that lasts for more than two to three weeks is the classic hallmark of pulmonary disease. Initially, this cough may be dry and unproductive, but as lung tissue breaks down, it gradually produces thick, discolored sputum.
Other vital systemic signs include:
- Drenching Night Sweats: This is a distinct clinical symptom where patients wake up in the middle of the night needing to change their clothes or bedding, even in cool environments.
- Unexplained Weight Loss: Chronic infection causes a prolonged inflammatory state, leading to a profound loss of appetite and muscle wasting.
- Unremitting Low-Grade Fever: The body maintains an elevated temperature, typically spiking in the late afternoon or evening.
- Hemoptysis (Coughing up Blood): In advanced cases, the destructive infection erodes local blood vessels within pulmonary cavities, causing streaks of blood or frank clots to appear in the sputum.
The Diagnostic Protocol
Securing an accurate diagnosis requires a combination of microbiological confirmation, imaging, and immunological screening. We can no longer rely on clinical symptoms alone.
1. Sputum Smear Microscopy
This traditional test involves collecting early morning sputum samples and staining them with special dyes (Acid-Fast Bacilli or AFB staining).
While it is rapid and affordable, it lacks high sensitivity, often missing infections where the bacterial load is low.
2. CBNAAT / GeneXpert
Cartridge Based Nucleic Acid Amplification Test (CBNAAT) has transformed modern diagnosis. This rapid molecular test identifies the DNA of the bacterium directly from sputum samples in under two hours.
Crucially, it also detects genetic resistance to Rifampicin, the most vital first-line medicine, allowing clinicians to tailor treatment regimens immediately.
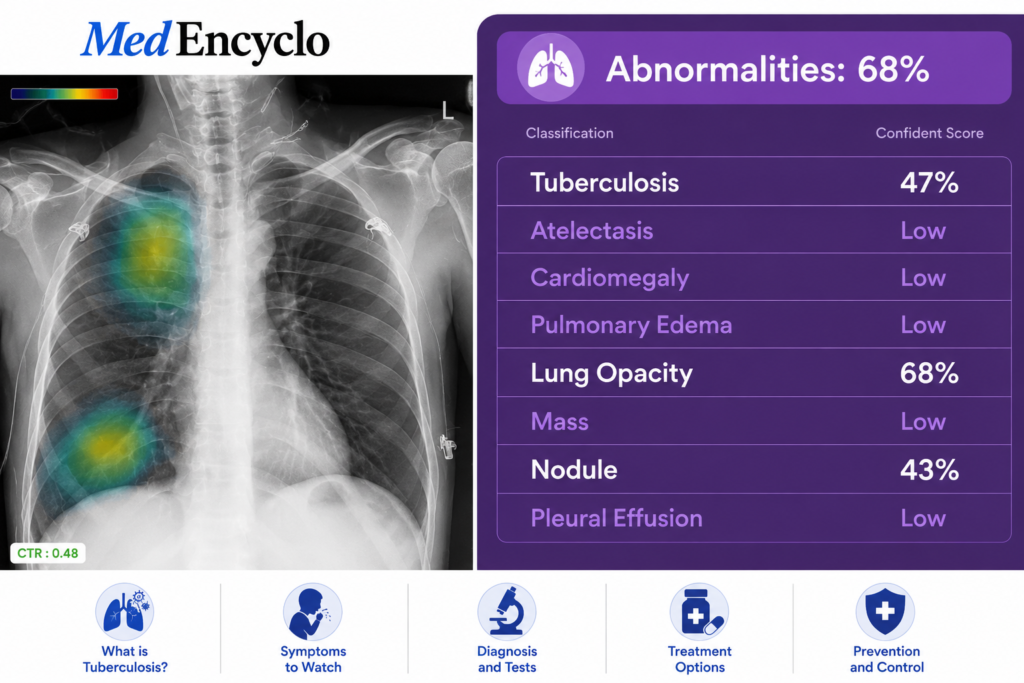
3. Chest X-ray
A chest X-ray provides an immediate look at structural damage.
In active disease, it frequently reveals patchy infiltrates, fluid accumulation around the lungs (pleural effusion), or distinct, hollowed-out spaces known as cavities, typically found in the upper sections of the lungs.
4. Mantoux Tuberculin Skin Test (TST)
This method involves injecting a small amount of purified protein derivative (PPD) just under the skin of the forearm. After 48 to 72 hours, a clinician measures the firm, raised bump that develops.
It is important to remember that a positive Mantoux test simply confirms that the body has encountered the bacteria; it cannot distinguish between a quiet latent infection and an active, contagious disease.
Potential Complications
Leaving an active infection untreated can lead to extensive tissue damage and life-threatening systemic complications.
- Permanent Lung Destruction: Chronic inflammation can destroy large sections of functional lung tissue, leaving behind deep scars, fibrotic lesions, and permanently dilated airways (bronchiectasis). This structural damage can cause chronic breathlessness long after the bacteria are gone.
- Systemic Dissemination: The bacteria can enter the bloodstream and seed other organ systems, leading to severe presentations like TB meningitis (infection of the brain linings) or Pott’s disease (destructive spinal infection).
- Drug-Resistant Strains: Inadequate or interrupted treatment allows the smartest bacteria to survive and mutate. This leads to Multi-Drug Resistant (MDR) or Extensively Drug-Resistant (XDR) strains, which require complex, second-line treatment regimens with higher toxicity profiles.
Clinical Treatment & Pharmacology
The primary goal of therapy is to completely eliminate the slow-growing bacteria while preventing the development of drug resistance. This goal cannot be achieved with a single medicine; it requires a coordinated, multi-drug strategy taken over a long period.
First-Line Anti-TB Medications
Standard treatment for a new case of drug-susceptible disease lasts for six months and is divided into two distinct phases.
The initial Intensive Phase lasts for two months and utilizes four powerful medications simultaneously to rapidly drop the bacterial load. This is followed by a four-month Continuation Phase using two core medications to eradicate any remaining dormant bacilli.
| Drug Name (Abbreviation) | Core Mechanism of Action | Common Side Effects | Critical Clinical Monitoring |
| Isoniazid (H) | Inhibits the synthesis of mycolic acids, disrupting the protective bacterial cell wall. | Peripheral neuropathy (numbness/tingling), hepatitis. | Co-administer Vitamin B6 (Pyridoxine) to protect nerve pathways. |
| Rifampicin (R) | Blocks bacterial RNA synthesis, halting replication. | Orange-red discoloration of body fluids, liver enzyme elevation. | Inform patients that colored tears and urine are harmless side effects. |
| Pyrazinamide (Z) | Targets dormant bacteria inside the acidic environment of host cells. | Hyperuricemia (gout flare-ups), joint pain, severe hepatotoxicity. | Monitor serum uric acid levels and baseline liver function. |
| Ethambutol (E) | Disrupts cell wall assembly, slowing bacterial growth. | Optic neuritis (decreased visual acuity, red-green color blindness). | Perform baseline and periodic visual acuity and color vision checks. |
The DOTS Strategy
To ensure patients successfully navigate this intensive six-month journey, international health bodies implement the Directly Observed Treatment, Short-course (DOTS) strategy.

Under this framework, a trained healthcare worker or community provider directly observes the patient swallowing each dose of medication. This structure prevents irregular dosing, provides immediate support for side effects, and ensures the patient completes the full course of treatment to prevent the rise of drug-resistant strains.
Prevention Strategies
Controlling this global health challenge requires a proactive approach built on vaccination, rapid infection control, and targeted preventive therapies.
The BCG Vaccine
The Bacillus Calmette-Guérin (BCG) vaccine is a live-attenuated vaccine administered at birth in countries with high disease prevalence.
While it does not reliably prevent adult pulmonary infection, it provides excellent protection for infants against severe, life-threatening pediatric presentations, such as military disease and bacterial meningitis.
Infection Control Measures
In healthcare settings and households managing active cases, simple environmental modifications can dramatically reduce transmission risk:
- Maximize Natural Ventilation: Keeping windows open and utilizing sunlight helps dilute droplet concentrations, as ultraviolet light naturally degrades suspended bacilli.
- Proper Cough Etiquette: Active patients should always use tissues or masks when coughing or sneezing to trap droplets before they enter the shared air.
- Prompt Isolation: Keeping infectious individuals in well-ventilated spaces until they complete their initial weeks of therapy helps break the chain of community transmission.
Red Flag Signs Requiring Urgent Care
While recovering at home on standard therapy, patients and caregivers must remain vigilant. Certain symptoms indicate severe disease progression or dangerous medication toxicity, requiring immediate emergency medical evaluation.
🚨 Seek Immediate Emergency Medical Treatment If You Experience:
- Severe, Progressive Breathlessness: Difficulty breathing or a rapid respiratory rate while resting.
- Massive Hemoptysis: Coughing up large amounts of bright red blood rather than simple dark streaks.
- Persistent, Uncontrolled Vomiting: Inability to retain medication, which can lead to rapid dehydration and treatment failure.
- Sudden Jaundice: Yellowing of the eyes or skin, dark urine, or severe right-sided abdominal pain, which indicate acute liver distress.
- Neurological Changes: High fever accompanied by a stiff neck, persistent confusion, or severe altered mental states.
Patient Education & Practical Recovery Tips
Successfully curing this infection requires open communication and shared accountability between the medical team and the patient.
The Danger of Premature Discontinuation
In clinical practice, we often see patients stop taking their medications after four to six weeks because their symptoms disappear, their appetite returns, and they feel fully recovered.
Stopping early is a dangerous mistake. While the active bacteria may be gone, the slow-growing, dormant bacilli remain hidden deep inside tissue granulomas.
Stopping treatment early allows these resilient strains to wake up, multiply, and return as a drug-resistant infection that is far more difficult and toxic to treat.
Nutritional Support
Fighting a chronic infection requires significant metabolic energy. Patients should focus on a nutrient-dense diet rich in proteins (such as lean meats, eggs, pulses, and dairy) to help rebuild lost muscle mass and strengthen cellular repair.
Avoiding alcohol is non-negotiable throughout the entire six-month journey, as mixing alcohol with anti-TB drugs places immense, dangerous stress on the liver.
Frequently Asked Questions (FAQs)
Is Tuberculosis fully curable?
Yes, standard drug-susceptible infections are completely curable in nearly all patients, provided the full course of multi-drug therapy is taken exactly as prescribed without missing doses.
How long does it take for a patient to stop being contagious?
In most clinical cases, a patient taking an effective drug combination sees a rapid drop in bacterial load and stops being contagious within two to three weeks of starting treatment. However, this must be confirmed by consecutive negative sputum tests.
What is the difference between MDR-TB and standard TB?
Standard cases respond well to inexpensive, first-line medications. Multi-Drug Resistant TB (MDR-TB) means the bacteria have mutated and can survive exposure to Isoniazid and Rifampicin, requiring longer, more complex second-line treatments.
Can someone get infected a second time after being cured?
Yes. Successfully completing treatment cures the current infection, but it does not grant permanent immunity. If an individual experiences prolonged exposure to an active case in the future, they can contract the disease again.
Why must I check my vision while taking Ethambutol?
Ethambutol can occasionally cause inflammation of the optic nerve, leading to blurred vision or difficulty distinguishing between red and green colors. Regular monitoring ensures that any early changes can be caught and managed by adjusting the medication.
Conclusion
Tuberculosis is a formidable health challenge, but it is completely curable when approached with accurate diagnostic tracking, timely treatment, and disciplined medication adherence.
If you or a loved one experiences a lingering cough, unexplained weight loss, or persistent night sweats, remember that early screening is your most effective tool.
By working closely with healthcare providers, utilizing supportive public health networks, and completing the prescribed treatment journey, we can successfully overcome this disease and build healthier, safer communities.
“This content is for informational and educational purposes only and is not intended as medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any medical decisions.”