Many people silently struggle with a heavy, persistent weight that eclipses their daily life, rendering even the simplest tasks monumental. This isn’t a temporary wave of the blues or a flaw in personal willpower. It is a genuine, treatable medical condition known as clinical depression.
Introduction
Depression is a profound public health challenge affecting more than 280 million people globally, according to data from the World Health Organization (WHO). In clinical practice, we have observed a sharp increase in these numbers over recent years.
In India, data from the National Mental Health Survey indicates that nearly 1 in 20 people live with this condition. Despite its massive prevalence, systemic stigma continues to isolate individuals, preventing them from accessing care.
It is important to understand that seeking mental health support is a profound act of courage and strength, not a admission of failure. Healing begins when we bring these silent struggles into the light of clinical understanding and genuine empathy.

What is Depression (MDD)?
Major Depressive Disorder (MDD) is a complex, multi-system mood disorder that fundamentally alters how a person thinks, feels, and navigates their environment. It extends far beyond the common human experience of transient sadness.
Sadness is an adaptive emotional reaction to loss, disappointment, or adversity. It comes in waves, allows for moments of joy, and gradually fades as time passes.
Clinical depression behaves entirely differently. It is an unremitting, pervasive state of low mood and loss of interest that persists for weeks, months, or years, significantly disrupting an individual’s ability to function at work, school, or home.
Causes & Risk Factors
In clinical psychology, we view MDD through the bio-psycho-social model. This perspective demonstrates that no single factor causes a mood disorder; instead, it arises from a dynamic interplay of elements:
- Biological Vulnerabilities: Having a first-degree relative with MDD elevates an individual’s personal risk by roughly three to four times.
- Psychological Traumas: Early childhood adversity, prolonged chronic stress, emotional neglect, or severe trauma can permanently sensitize the brain’s stress response networks.
- Social and Environmental Triggers: Sudden isolation, financial crises, toxic relationships, or significant life transitions can break down a person’s psychological reserves.
- Co-occurring Medical Issues: Living with chronic pain, stroke, neurological disorders, or conditions like Insomnia can actively exhaust a person’s coping capacity.
The Pathophysiology Behind the Pain
To understand what happens during clinical depression, it helps to look inside the brain’s delicate messaging infrastructure. Historically, medicine viewed it as a simple “chemical imbalance.” Today, we understand it is actually a disruption in neural network connectivity and neuroplasticity.
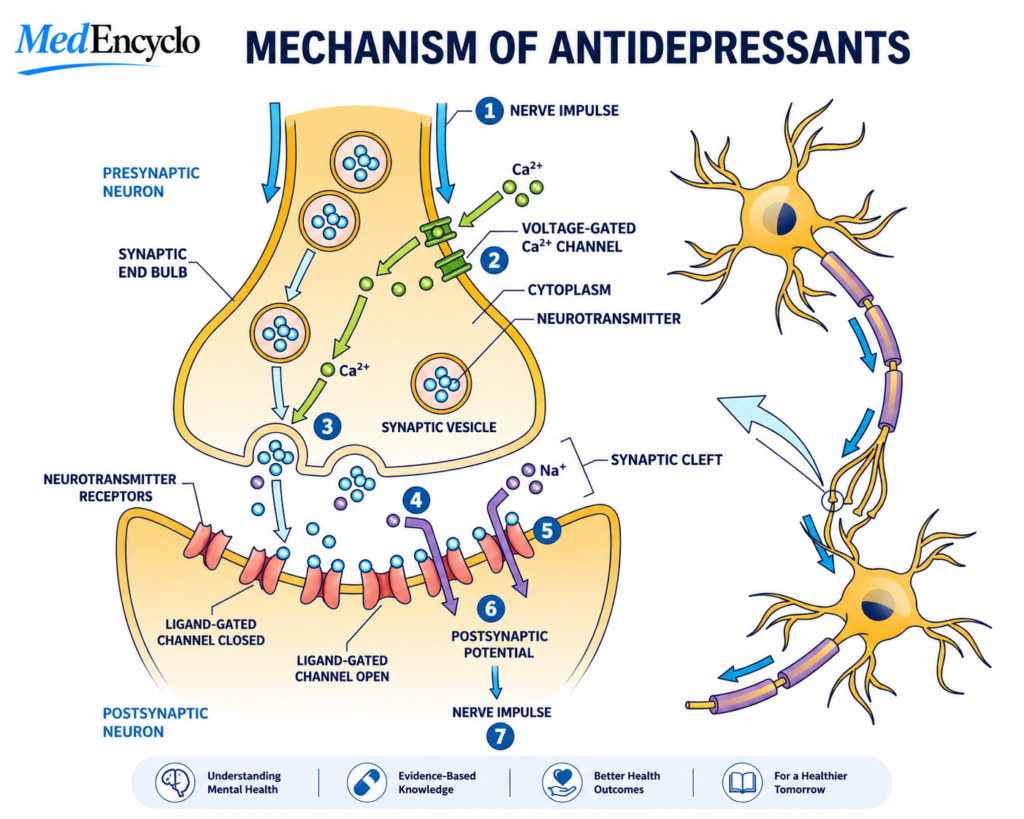
Think of the brain as a massive city power grid. In a healthy brain, tiny chemical messengers called neurotransmitters—primarily serotonin, norepinephrine, and dopamine—ensure that signals flow smoothly across synapses.
- Serotonin helps regulate mood, sleep patterns, and emotional resilience.
- Norepinephrine influences alertness, physical energy, and cognitive focus.
- Dopamine drives our sense of reward, motivation, and physical pleasure.
When a person experiences MDD, this communication network experiences a systemic brownout. Signals stall, neural pathways in the prefrontal cortex shrink, and the amygdala—the brain’s emotional alarm system—becomes overactive. This biological shift makes it incredibly difficult to feel joy or maintain balanced perspective.
Recognizing the Signs & Symptoms
The Diagnostic and Statistical Manual of Mental Disorders (DSM-5) requires at least five symptoms to be present during the same two-week period for a formal clinical diagnosis. At least one of these symptoms must be a depressed mood or a marked loss of interest or pleasure (anhedonia).
Emotional Symptoms
- A pervasive feeling of sadness, emptiness, or tearfulness.
- Anhedonia: An inability to feel pleasure from hobbies, passions, or loved ones.
- Feelings of profound worthlessness, inappropriate guilt, or self-loathing.
Physical & Vegetative Symptoms
- Chronic fatigue and depleted energy levels, making basic tasks feel exhausting.
- Significant changes in sleep patterns, such as severe Insomnia or sleeping too much (hypersomnia).
- Appetite disruptions, leading to rapid, unintended weight loss or weight gain.
Cognitive Symptoms
- Sustained difficulty thinking, concentrating, or making minor daily choices.
- Psychomotor agitation or noticeable slowing of speech and physical movement.
- Recurrent thoughts of death, suicidal ideation, or self-harm.
The Different Faces of Depression
Depression does not present identically in every person. It manifests in several distinct clinical forms:
| Type of Depressive Disorder | Primary Clinical Features | Typical Presentation |
| Major Depressive Disorder (MDD) | Discrete, severe episodes lasting at least 2 weeks. | Pervasive low mood, acute functional impairment. |
| Persistent Depressive Disorder (Dysthymia) | A chronic, low-grade depressive state lasting at least 2 years. | Functions reasonably well but feels a constant gray pall over life. |
| Peripartum (Postpartum) Depression | Onset occurs during pregnancy or in the weeks following childbirth. | Intense anxiety, exhaustion, and difficulty bonding with the newborn. |
| Seasonal Affective Disorder (SAD) | Depressive episodes tied directly to seasonal changes. | Typically begins in autumn and resolves during spring/summer. |
How is Depression Diagnosed?
There is no blood test or brain scan that can definitively diagnose clinical depression. Instead, diagnosis relies on a thorough, structured evaluation by a qualified mental health professional.
The clinical assessment begins by ruling out primary organic medical causes. Conditions like hypothyroidism, severe Vitamin D or B12 deficiencies, and autoimmune diseases can mimic a depressive episode.
Clinicians frequently utilize validated screening tools like the Patient Health Questionnaire-9 (PHQ-9) to gauge symptom severity. However, these scales serve as guides; they never replace a detailed diagnostic interview that reviews an individual’s personal history, lifestyle, and unique struggles.
Potential Complications
Left unmanaged, clinical depression can gradually erode multiple areas of a person’s life:
- Social Isolation: Individuals often pull away from their support networks, fracturing marriages, friendships, and family structures.
- Occupational Impairment: Absenteeism, cognitive fog, and dropped responsibilities can lead to job loss or academic failure.
- Substance Abuse: Many people turn to alcohol or unprescribed substances to self-medicate, which ultimately worsens the underlying neural distress.
- Physical Health Decline: Chronic depression elevates cortisol levels, compounding the risks for cardiovascular diseases, diabetes, and immune dysfunction.
Comprehensive Management & Treatment
The most effective, evidence-based approach to treating MDD typically combines targeted psychological therapy with appropriate medical interventions and lifestyle changes.

A. Psychotherapy
Psychotherapy serves as a cornerstone of long-term recovery. In clinical practice, two modalities stand out:
- Cognitive Behavioral Therapy (CBT): This approach helps individuals identify, challenge, and replace maladaptive thought patterns and core negative beliefs.
- Interpersonal Therapy (IPT): This framework focuses on improving relationship dynamics, resolving unresolved grief, and navigating difficult life role transitions.
B. Pharmacotherapy (Medications)
From a clinical pharmacy standpoint, modern antidepressants are highly effective tools designed to restore neural network communication.
Important Pharmacist Note: Antidepressants are not addictive, and they do not change your fundamental personality. They require patience, as they typically take four to six weeks of consistent daily use to reach full therapeutic effectiveness.
- Selective Serotonin Reuptake Inhibitors (SSRIs): Medications like Fluoxetine, Sertraline, and Escitalopram work by increasing available serotonin levels in the synaptic cleft.
- Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs): Agents like Duloxetine and Venlafaxine target both serotonin and norepinephrine to treat cases accompanied by severe fatigue or chronic pain.
C. Evidence-Based Lifestyle Measures
Lifestyle adjustments serve as powerful allies alongside clinical treatment. Regular aerobic exercise triggers the release of Brain-Derived Neurotrophic Factor (BDNF), a protein that stimulates neuroplasticity and repairs damaged neural pathways.
Prioritizing structured sleep routines, avoiding alcohol, and maintaining basic social interactions help stabilize circadian rhythms and prevent symptom recurrence.
Prevention & Early Intervention
While we cannot always prevent depression entirely, we can significantly reduce the severity of subsequent episodes through early intervention:
- Build Emotional Literacy: Learn to identify your personal early signs of distress, such as shifts in irritability, sleep disruption, or minor withdrawal.
- Practice Boundary Setting: Learn to manage professional and personal demands to prevent chronic burnout.
- Cultivate Low-Friction Support Systems: Maintain a small group of trusted individuals who understand your mental health history without judgment.
Red Flag Signs: When to Seek Immediate Help
It is crucial to recognize when a depressive episode shifts from a state of low mood into an acute mental health emergency:
- Explicitly speaking about or planning suicide, death, or self-harm.
- An abrupt, unexplained shift from deep despair to absolute calm or euphoria (which can signal a finalized decision to self-harm).
- Engaging in dangerous, impulsive, or reckless behaviors.
- Withdrawing entirely from all human contact or giving away valued personal possessions.
Patient & Caregiver Guidance
Supporting a family member or loved one living with clinical depression requires balance, steady patience, and deep empathy.
What to Do:
- Listen patiently without rushing to offer easy fixes or solutions.
- Offer low-stress, practical help with daily tasks like grocery shopping, cooking, or arranging medical appointments.
- Gently remind them that their current state is a temporary symptom of a treatable condition, and that they will not always feel this way.
What Not to Say:
- “Just think positively and snap out of it.”
- “You have so much to be grateful for, why are you sad?”
- “You’re just choosing to look at the negative side of things.”
Frequently Asked Questions
Is depression a lifelong condition?
Not necessarily. For many individuals, depression manifests as episodic, meaning they experience distinct periods of illness followed by complete recovery. For others, it can be a chronic challenge that requires long-term management, much like managing hypertension or diabetes.
How long do I need to stay on antidepressant medications?
In a typical first episode of depression, clinical guidelines recommend continuing antidepressant therapy for six to nine months after you feel fully recovered. This prevents immediate relapse. For recurrent cases, your doctor may suggest longer-term maintenance therapy.
What should I do if my current medication isn’t working?
It is very common to try more than one medication before finding the right fit. If you don’t feel an improvement after four to six weeks, talk to your doctor or pharmacist. They can adjust your dosage, switch you to a different class of medication, or add an augmenting agent. Never stop taking your medication abruptly.
Can a poor diet cause depression?
While a poor diet alone does not cause a clinical mood disorder, research shows a strong link between systemic inflammation, gut health, and brain health. A balanced diet rich in whole foods, omega-3 fatty acids, and antioxidants supports overall brain function and complements your standard treatment plan.
How can I distinguish between grief and clinical depression?
Grief typically occurs in waves and centers around thoughts of a specific loss. While painful, a grieving person’s self-esteem usually remains intact. In contrast, clinical depression is an unremitting blanket of low mood that isn’t always tied to a loss, and it is almost always accompanied by feelings of worthlessness and self-criticism.
Conclusion
Depression can make you feel entirely isolated from the rest of the world, but you do not have to carry this weight alone. With the right combination of psychotherapy, medical guidance, and supportive relationships, recovery is fully achievable.
If you or a loved one are struggling, reach out to a certified mental health professional or a local crisis helpline today. Taking that first step toward care can open the door to true healing.
“This content is for informational and educational purposes only and is not intended as medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any medical decisions.”