Osteoarthritis is the most common form of arthritis worldwide, affecting millions of individuals and serving as a leading cause of chronic disability. Often referred to simply as “wear-and-tear” arthritis, it occurs when the protective tissue at the ends of your bones gradually erodes over time.
In my clinical practice, I hear variations of the same story every week: a patient notices a dull, aching deep within their knee after a long walk, or experiences a stubborn morning stiffness that makes getting out of bed feel like a monumental task. While we traditionally view this as a condition of the elderly, the epidemiological landscape is shifting rapidly.
Today, a sedentary lifestyle, rising obesity rates, and sports-related joint trauma mean that we are diagnosing this degenerative joint disease in younger adults far more frequently than we did a few decades ago. Understanding this condition early is the single best way to preserve your long-term mobility.
What is Osteoarthritis?
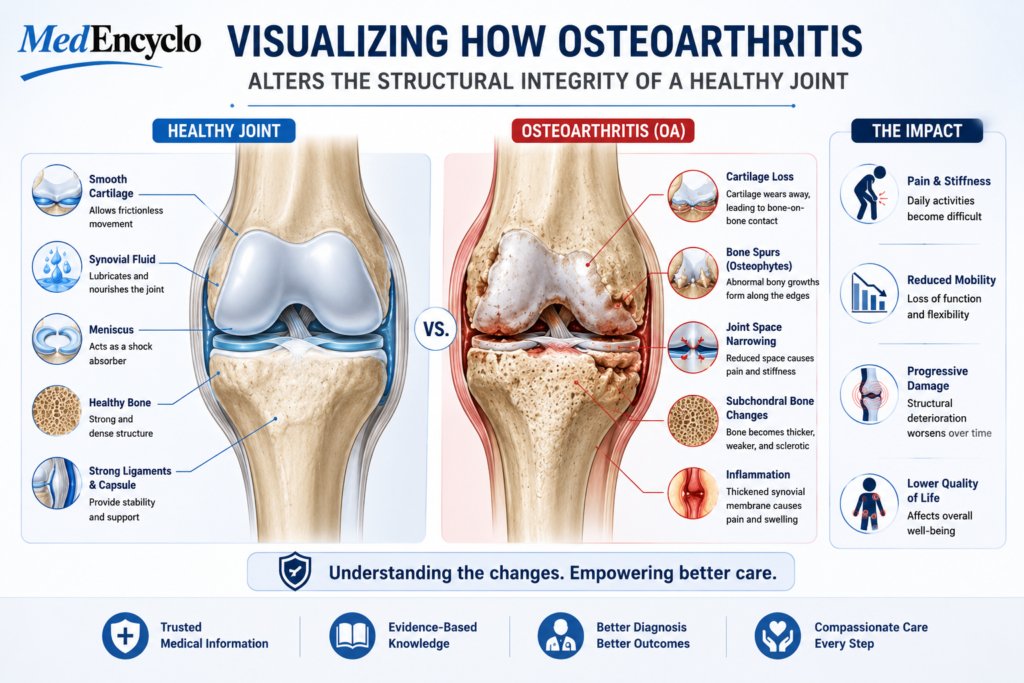
To understand osteoarthritis, it helps to picture a smoothly functioning machine. In a healthy dynamic joint, the ends of the meeting bones are capped with a slick, rubbery substance called articular cartilage. This cartilage acts as a frictionless shock absorber, allowing your bones to glide over one another seamlessly during movement.
When a patient develops this condition, this protective cartilage begins to fray, thin, and degenerate. It is not just an isolated disease of the cartilage, however; it is a disease of the entire joint complex, including the underlying bone, the joint lining (synovium), the ligaments, and the surrounding muscles.
While it can develop in virtually any joint, it most frequently attacks the weight-bearing and highly repetitive-use structures:
- Knees: The most common site, resulting in severe pain during walking, climbing stairs, or squatting.
- Hips: Causing a deep, nagging groin or buttock pain that can significantly limit your stride length.
- Spine: Usually presenting as localized stiffness and aching in the lower back (lumbar spine) or neck (cervical spine).
- Hands: Targeting the base of the thumb and the furthest finger joints, often leading to visible bony bumps and difficulty with fine motor skills like buttoning a shirt.
Unlike systemic inflammatory conditions such as Rheumatoid Arthritis, which is an autoimmune disease where the body mistakenly attacks its own tissues, this condition is primarily localized and driven by mechanical stress and cellular degradation within the specific joint.
The Primary Causes and Risk Factors
Many patients believe that getting arthritis is simply an unavoidable consequence of turning a certain age. While aging is certainly a prominent variable, the development of this condition is multifactorial. Several distinct risk factors dictate how quickly your joints age.
[Mechanical Stress / Excess Weight] + [Age / Genetics]
│
▼
[Cartilage Wear & Micro-Tears]
│
▼
[Osteoarthritis Development]Ageing
As the body matures, the natural water content of the cartilage decreases, and its protein structure becomes more brittle. The body’s innate ability to repair minor micro-cracks in the cartilage template slows down, making the joint progressively more vulnerable to everyday stress.
Obesity
Carrying excess body weight is a massive accelerant for joint wear. From a purely mechanical standpoint, every extra kilogram of weight you carry translates to roughly four kilograms of additional pressure across your knees when you take a step.
Furthermore, fat tissue is metabolically active. It releases systemic inflammatory proteins called adipokines, which travel through your bloodstream and actively accelerate the chemical breakdown of cartilage tissue throughout your body, including your hands. Managing Obesity is one of our primary therapeutic goals in joint preservation.
Joint Injury or Overuse
If you suffered a severe ligament tear, meniscus injury, or a bone fracture near a joint during your youth, the baseline mechanics of that joint are permanently altered. Even after a successful surgical repair, the uneven weight distribution can lead to post-traumatic arthritis decades later. Similarly, repetitive occupational hazards—such as prolonged kneeling or heavy lifting—can prematurely wear down specific joints.
Genetics
Your DNA dictates the structural composition of your collagen and the precise alignment of your skeleton. If your parents or siblings suffered from severe joint issues early in life, you may have inherited minor structural variations or cartilage vulnerabilities that predispose you to similar challenges.
Sedentary Lifestyle
Muscles act as the secondary stabilization system for your skeletal system. When you lead a highly sedentary life, the quadriceps, hamstrings, and gluteal muscles weaken. Without muscular support, your joints absorb the entirety of every impact shock, hastening the structural decline.
The Pathophysiology: What is Happening Inside Your Joint?
To clearly understand what is happening inside an arthritic joint, consider a simple clinical analogy: imagine a premium, thick mattress that gradually loses its inner padding.
Initially, the surface of your articular cartilage is perfectly smooth. Over time, due to mechanical stresses, microscopic cracks form on this surface. As you continue to walk and move, these micro-tears deepen. The cartilage begins to flake off into the joint space, leaving behind a rough, uneven texture.
Healthy, Smooth Cartilage
│
▼
Microscopic Surface Fraying
│
▼
Deep Cartilage Erosion & Thinning
│
▼
Bone-on-Bone Friction & Osteophyte FormationAs the cushion wears out completely, the underlying bones lose their protection and begin to rub directly against one another. This raw bone-on-bone friction creates immense pressure. In response, the body attempts to heal itself by increasing the surface area of the joint. It does this by growing abnormal, jagged bony projections at the margins of the joint, known as osteophytes or “bone spurs.”
Simultaneously, pieces of loose cartilage can irritate the delicate inner lining of the joint capsule (the synovium), causing a secondary, localized inflammatory response that brings fluid accumulation, swelling, and a deep, throbbing ache.
Recognizing the Signs and Symptoms
The onset of symptoms is typically insidious, developing slowly over several months or years. Many patients ignore the earliest warning signs, attributing them to simple fatigue. Recognizing these signals early can drastically improve your treatment outcomes.
- Joint Pain During Activity: The hallmark symptom is a deep, dull ache localized to the joint. In the early stages, this pain surfaces during or after prolonged physical activity and resolves completely with rest. As the condition advances, the pain becomes more persistent and can eventually disrupt your sleep.
- Brief Morning Stiffness: You may experience a distinct tightness when first waking up or after sitting watching television for an hour. Crucially, this morning stiffness typically lasts less than 30 minutes. If stiffness persists for hours, it points toward an inflammatory autoimmune condition rather than mechanical wear.
- Reduced Range of Motion: You might find it increasingly difficult to bend your knee fully to squat, sit cross-legged on the floor, or extend your arms over your head comfortably.
- Crepitus: This is a distinct grating, cracking, or popping sensation felt or heard when you move the affected joint. It is caused by the rough, damaged surfaces rubbing against each other.
- Localized Swelling: While not as pronounced as in inflammatory systemic arthritis, mild soft-tissue swelling or a “boggy” feeling can occur due to excess synovial fluid production inside the joint capsule.
How We Diagnose Osteoarthritis in the Clinic
When you visit a specialist, arriving at an accurate diagnosis involves a systematic blend of your medical history, a targeted physical exam, and objective imaging. There is no definitive blood test for this condition, though we often run lab panels to rule out metabolic gout or rheumatoid factors.
Clinical Examination
Your physician will carefully palpate the joint lines, checking for localized tenderness, warmth, and bony enlargements. We assess your passive and active range of motion, look for signs of ligament instability, and carefully evaluate your gait (the way you walk) to see if you are compensating for pain.
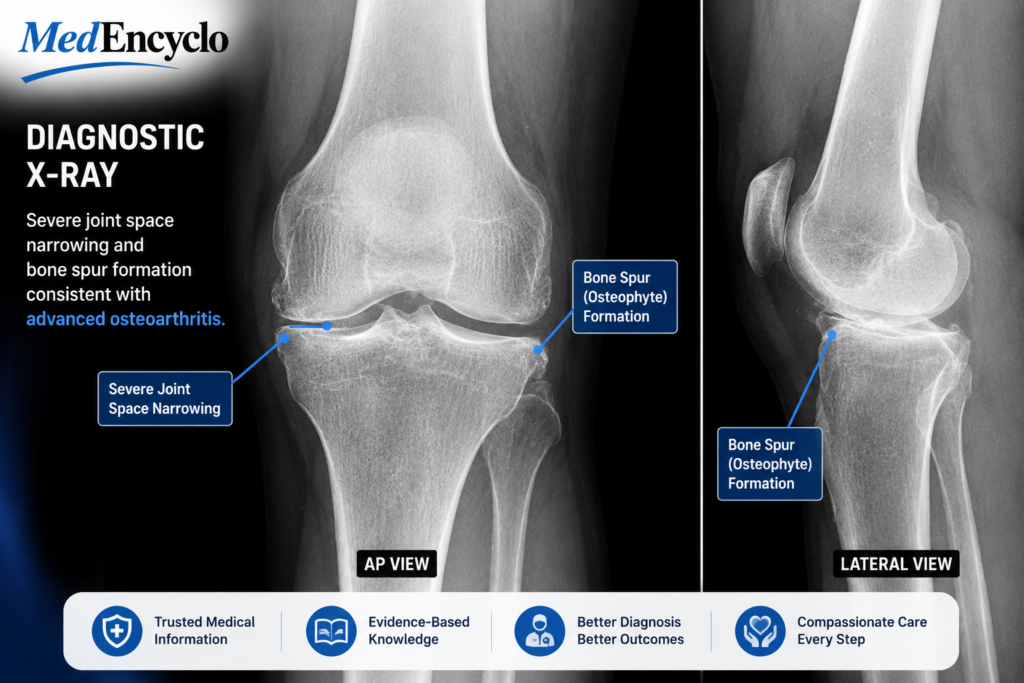
Plain X-ray Findings
A simple, weight-bearing X-ray remains our gold standard diagnostic tool. In a healthy joint film, the space between the bones appears clear and wide because the cartilage is invisible on radiography. In an arthritic joint, we look for four classic radiological hallmarks:
| X-Ray Hallmark | What it Indicates |
| Joint Space Narrowing | Significant loss and thinning of the protective cartilage cushion. |
| Osteophytes | Bone spurs forming at the joint margins in response to friction. |
| Subchondral Sclerosis | Thickening and hardening of the bone directly beneath the damaged cartilage. |
| Subchondral Cysts | Small, fluid-filled pockets forming inside the bone matrix due to chronic stress. |
When is an MRI Needed?
In clinical practice, we rarely order an MRI for a routine case. However, an MRI becomes invaluable if your symptoms do not match your plain X-rays, if we suspect an acute meniscus or ligament tear alongside the wear, or if we need to evaluate the early stages of bone marrow edema that standard X-rays miss.
Potential Complications of Neglected Joint Health
Ignoring chronic joint degradation can set off a cascading effect that extends far beyond physical discomfort.
- Chronic Pain Syndrome: Persistent pain alters the way your central nervous system processes pain signals, sometimes leading to central sensitization, where even minor movements trigger severe discomfort.
- Progressive Loss of Mobility: As moving hurts, patients naturally move less. This creates a vicious cycle of muscle wasting, joint contractures, and a severe loss of functional independence.
- Secondary Metabolic Decline: When severe knee or hip pain prevents you from walking, your sedentary hours skyrocket. This inactivity directly increases your risk for cardiovascular disease, poorly controlled type 2 diabetes, and rapid weight gain.
- Sleep Disturbances and Mood Disorders: Nocturnal joint pain severely disrupts restorative sleep cycles, which strongly correlates with clinical depression, anxiety, and a diminished overall quality of life.
Comprehensive Management Strategies
Managing this condition effectively requires a multi-layered, individualized treatment pyramid. There is currently no magic cure to instantly regenerate vanished cartilage, but we have an array of highly effective strategies to stop its progression, control your pain, and preserve your active lifestyle.
[ Surgical Options ] <-- Advanced (Joint Replacement)
[ Physiotherapy & Meds ] <-- Intermediate (NSAIDs, Bracing)
[ Lifestyle Modifications ] <-- Foundational (Weight Loss, Low-Impact Exercise)A. Lifestyle Modifications
This forms the foundational base of our treatment pyramid. Without these changes, advanced medical interventions provide only temporary relief.
- Strategic Weight Loss: Dropping even 5% of your total body weight can reduce joint stress by up to 20%, dramatically reducing daily pain scores.
- Low-Impact Aerobic Exercise: You must keep moving to keep the joint lubricated. Fluid movement pumps vital nutrients into the remaining cartilage matrix. Swap high-impact running or jumping for joint-friendly alternatives like swimming, water aerobics, stationary cycling, or elliptical training.
B. Pharmacotherapy and Supplements
As a clinical pharmacist and physician team, our medication motto is clear: use the lowest effective dose for the shortest duration possible to maintain safety.
- Topical Analgesics: This is always our first line of defense, especially for accessible joints like the knees and hands. Topical Diclofenac gels, patches, or capsaicin creams penetrate deep into local tissues, providing targeted pain relief without passing through your stomach or kidneys.
- Paracetamol (Acetaminophen): Useful for mild, intermittent baseline pain, but it does not address localized inflammation.
- Oral NSAIDs (Non-Steroidal Anti-Inflammatory Drugs): Medications such as Ibuprofen, Naproxen, or selective COX-2 inhibitors like Celecoxib are highly effective for moderate-to-severe flare-ups. However, prolonged oral use requires strict medical supervision, as it can cause gastrointestinal ulcers, elevate blood pressure, and strain kidney function.
- Glucosamine and Chondroitin Supplements: One common concern among patients is whether these popular supplements actually work. The clinical evidence from large-scale trials remains mixed. While they do not reliably regrow lost cartilage, some patients experience mild symptomatic relief. It is generally safe to try high-quality formulations for 2–3 months; if you notice no distinct benefit by then, it is best to discontinue them and save your financial resources.
C. Physiotherapy and Rehabilitation
A customized course of targeted Physiotherapy is arguably your most powerful non-surgical weapon. A skilled physical therapist will focus intensely on strengthening the dynamic stabilizers of your joints.
For the knee, this means building up the quadriceps and hamstring muscles. For the hip, the focus turns to the gluteal medius and core muscles. Therapists also employ stretching protocols to combat joint stiffness and utilize neuromuscular training to correct biomechanical walking imbalances.
D. Surgical Interventions
When conservative therapies fail to provide relief, and your structural independence is profoundly compromised, we explore surgical options.
- Intra-Articular Injections: If oral medications aren’t enough, we can inject a corticosteroid directly into the joint space for rapid, temporary relief of severe inflammation. Alternatively, hyaluronic acid injections (viscosupplementation) act as a synthetic lubricant, though results vary from patient to patient.
- Total Joint Replacement (Arthroplasty): For end-stage, bone-on-bone degradation, a total knee or hip replacement is highly effective. In this procedure, the damaged bone ends are precision-resurfaced with advanced medical-grade metals and high-density plastics. Modern surgical techniques allow for rapid recovery, often getting patients up and walking on the very same day as the procedure.
Practical Home Remedies and Self-Care
While clinical therapies are essential, what you do in your own home on a daily basis matters immensely.
- The Power of Alternating Temperature: Use Heat Therapy (such as warm baths or heating pads) for 15–20 minutes in the morning to relax tight muscles, increase local blood flow, and soothe stiff joints. Use Cold Therapy (like an ice pack wrapped cleanly in a towel) for 15 minutes after activities or at the end of the day to numb acute pain and reduce local swelling.
- Smart Activity Modification: Learn to pace your daily activities. If you have a large home project, break it into smaller 20-minute segments interspersed with brief periods of seated rest. Avoid sitting in low, deep sofas that place extreme mechanical strain on your hips and knees when standing up.
- Asscriptive Devices: Do not view a walking cane or a structural knee brace as a sign of weakness; view it as an assistive tool that offloads joint pressure, preserves your remaining cartilage, and significantly improves your walking stamina.
Proactive Prevention: Guarding Your Joints Early
You can actively reduce your risk of developing severe joint degeneration by making intentional choices today:
- Wear Supportive Footwear: Invest in shoes that provide adequate arch support and shock absorption to ensure forces are distributed evenly across your lower joints.
- Maintain a Lean Body Mass Index (BMI): Keeping your weight within a healthy target range is the single most definitive action you can take to shield your lower extremity joints from premature wear.
- Cross-Train Your Fitness Routine: Avoid performing the exact same high-impact repetitive exercise day after day. Blend strength training with flexibility and low-impact cardio.
- Prioritize Ergonomic Adjustments: Ensure your workplace setup, desk height, and chair support promote neutral skeletal alignment, reducing continuous micro-stress on your spine and hips.
Red Flag Signs: When to See Your Doctor Immediately
While this is typically a slowly progressive condition, certain symptoms warrant urgent medical evaluation:
- Sudden Inability to Bear Weight: If a joint suddenly gives out or completely locks up, preventing you from walking even a few steps.
- Signs of Acute Infection: If a single joint rapidly becomes intensely hot to the touch, red, severely swollen, and is accompanied by a fever or chills (this could indicate a life-threatening septic joint).
- Rapid Functional Loss: A sudden drop in your ability to perform basic daily activities, or new, severe shooting numbness or tingling down your legs or arms, indicating severe spinal nerve compression.
Patient Education: Essential Tips for Daily Life
Living well with this condition requires shifting from a mindset of fear to one of proactive structural management.
- Remember that Motion is Lotion: Avoid long, uninterrupted periods of total couch rest. Inactivity causes the synovial fluid inside your joints to thicken, making your subsequent movements far more painful. Set a timer to stand up, stretch, and walk around for two minutes every hour.
- Commit to Medication Adherence Safely: Never arbitrarily double your dose of pain relievers on a bad day without consulting your clinical pharmacist or physician, as this significantly increases your risk of internal organ toxicity.
- Listen to Your Body’s Signals: There is a distinct difference between the healthy, burning muscular discomfort of exercise and the sharp, piercing structural pain of a joint under too much stress. If an activity causes sharp pain that lasts for more than 24 hours, it is a clear sign to scale back the intensity.
Frequently Asked Questions (FAQs)
Is osteoarthritis the same thing as osteoporosis?
No, these are entirely distinct skeletal conditions, though both are common with age. Osteoarthritis is a mechanical disease of the joint structures and cartilage wear. Osteoporosis is a silent disease of the bone tissue itself, where bones lose mass and density, making them fragile and highly susceptible to fractures.
Can dynamic exercise actually damage my joints further if I have arthritis?
Many patients notice that high-impact activities like running can exacerbate their symptoms. However, appropriate low-impact exercises—such as swimming, elliptical training, and targeted quadriceps strengthening—will actually protect your joints. It achieves this by strengthening the surrounding muscular support and improving joint lubrication.
Why do my joints feel so much more painful when the weather changes or before it rains?
This is a very common observation in clinical practice. When atmospheric barometric pressure drops (which often happens right before a storm or rain), the tissues and fluids within your compromised joint capsule can expand slightly. Because an arthritic joint is highly sensitive, this pressure change directly irritates local nerve endings, resulting in a perceptible flare-up of stiffness and ache.
Are there any specific foods or strict diets I should follow to cure this condition?
There is no specific diet that will magically cure or reverse cartilage loss. However, adopting a highly nutritious, anti-inflammatory Mediterranean diet—rich in leafy greens, berries, olive oil, nuts, and omega-3 fatty acids (found in fish like salmon)—can help naturally reduce systemic inflammatory markers and aid in healthy weight management.
At what point should I stop conservative treatment and consider a total joint replacement?
You should seriously discuss joint replacement surgery with an orthopedic specialist when conservative options (medications, physiotherapy, weight loss, and injections) no longer provide acceptable relief, and your severe pain consistently disrupts your sleep or prevents you from performing foundational daily activities like walking or bathing.
Conclusion
Experiencing osteoarthritis does not mean you have to accept a steady decline into a sedentary life or give up the activities you love. While cartilage degeneration cannot be instantly undone, it is a highly manageable condition when approached proactively.
By prioritizing strategic weight management, staying committed to joint-friendly low-impact movement, utilizing targeted therapies, and partnering closely with your medical team, you can effectively minimize pain and protect your long-term mobility. Take charge of your joint health today; your body will thank you for years to come.
For additional evidence-based medical information and global support resources regarding joint health, please explore the official portals of the World Health Organization (WHO), the Centers for Disease Control and Prevention (CDC), and the Arthritis Foundation.
“This content is for informational and educational purposes only and is not intended as medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any medical decisions.”