Introduction
Acne vulgaris, commonly known as pimples or simply acne, is a chronic, inflammatory dermatological condition affecting the pilosebaceous units (hair follicles and associated oil glands). Far from being a mere cosmetic nuisance, it is a complex medical condition that can profoundly impact an individual’s quality of life.
Statistically, acne is one of the most prevalent skin conditions globally. It affects up to 85% of adolescents and young adults aged 12 to 24. However, its reach extends well into adulthood; post-adolescent acne is increasingly diagnosed, particularly in women.
Acne occurs when a perfect storm of biological factors—primarily excess oil, dead skin cells, and targeted bacterial growth—converges to clog pores and trigger an inflammatory response deep within the skin.
Types of Acne Lesions
Understanding the specific types of acne lesions is critical, as clinical management relies directly on classifying what is presenting on the skin. Acne lesions are fundamentally divided into non-inflammatory and inflammatory types.
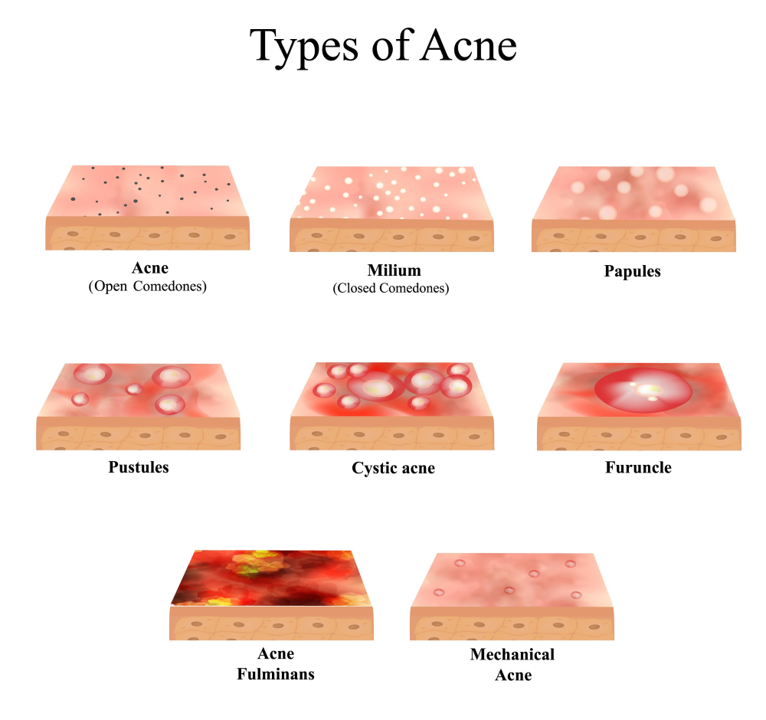
Acne (Open Comedones)
The first type shown is acne characterized by open comedones, commonly known as blackheads. These are small bumps on the skin that are open to the surface, and the dark appearance is due to the oxidation of melanin and sebum.
Milium (Closed Comedones)
Next is milium, or closed comedones, also known as whiteheads. These are similar to blackheads but the pore is closed, trapping the sebum and dead skin cells beneath the surface, creating a small white or flesh-colored bump.
Papules
Papules are a more inflammatory form of acne. They appear as small, red, tender bumps without a pus-filled head. This occurs when the walls of the hair follicles break down from inflammation.
Pustules
Following papules, we have pustules, which are what most people think of as pimples. They are similar to papules but have a visible white or yellow pus-filled center. The pus is a mixture of dead white blood cells, bacteria, and other debris.
Cystic acne
Cystic acne is a more severe form, characterized by large, painful, pus-filled cysts that form deep within the skin. These can be very painful and are more likely to cause scarring.
Furuncle
A furuncle, commonly known as a boil, is a deep infection of the hair follicle. It starts as a red, tender lump and grows larger as it fills with pus. A carbuncle is a cluster of furuncles.
Acne Fulminans
Acne fulminans is a rare and severe form of cystic acne that suddenly appears. It is characterized by inflammatory and ulcerative nodules and is often accompanied by systemic symptoms like fever and joint pain.
Mechanical Acne
Finally, mechanical acne is caused by heat, friction, and pressure against the skin. This can be from items like helmets, chin straps, or tight clothing, which can irritate the skin and lead to breakouts.
Non-Inflammatory Lesions
- Open Comedones (Blackheads): These occur when a pore is partially blocked by sebum and dead keratinocytes. The surface remains open to the air, causing the trapped melanin and lipids to oxidize and turn black or dark brown.
- Closed Comedones (Whiteheads): These form when the pore blockage is completely sealed beneath the skin’s surface. Because the contents are not exposed to oxygen, they appear as small, flesh-colored or white bumps.
Inflammatory Lesions
- Papules: Small, raised, solid red or pink bumps that feel tender to the touch. They signal that inflammation has begun to break down the follicular wall.
- Pustules: Similar to papules, but topped with a visible collection of pus (white blood cells) at the center.
- Nodules: Large, solid, painful lumps lodged deep within the dermis. They develop when a clogged follicle ruptures deeply into the surrounding tissue.
- Cysts: Deep, fluid-filled, painful lesions that carry a high risk of permanent tissue damage and scarring. They represent the most severe manifestation of acne vulgaris.
Acne Causes & Risk Factors
The development of acne is rarely dictated by a single factor. Instead, a combination of systemic and environmental triggers determines its onset and severity.
Primary Drivers
- Hormonal Fluctuations: Surges in androgens (male hormones present in both men and women) during puberty, menstrual cycles, and pregnancy stimulate the sebaceous glands to enlarge and overproduce oil.
- Excess Sebum Production: Overactive oil glands create an environment where dead skin cells stick together rather than shedding normally.
- Bacterial Involvement (Cutibacterium acnes): This anaerobic bacterium thrives naturally in the oily environment of the skin. When trapped inside a blocked pore, it multiplies rapidly, releasing metabolic byproducts that irritate the skin.
- Genetics: Family history is a powerful predictor. If both parents suffered from severe acne, their children are significantly more likely to develop it.
Secondary Triggers and Exacerbating Factors
- Diet: Modern clinical evidence suggests that diets with a high glycemic index (processed carbohydrates, sugary foods) and high consumption of skim dairy products can elevate insulin-like growth factor 1 (IGF-1), worsening breakouts.
- Stress: While stress does not directly cause acne, it releases cortisol and neuroinflammatory modulators that exacerbate underlying inflammation.
- Cosmetics and Skincare: Heavy, oil-based, or comedogenic makeup and sunscreens can mechanically block pores.
- Medications: Certain drugs, including systemic corticosteroids, lithium, anticonvulsants, and anabolic steroids, can induce acneform eruptions.
Pathophysiology
The lifecycle of a pimple unfolds through a precise, four-step pathogenic pathway within the pilosebaceous unit.
- Follicular Hyperkeratinization: The lining of the hair follicle sheds skin cells abnormally fast. These cells stick together, forming a dense plug (microcomedone) that seals the pore.
- Sebum Overproduction: Under androgenic stimulation, sebaceous glands pump excess lipids into the microcomedone, filling the trapped space.
- Bacterial Proliferation: The anaerobic, lipid-rich environment creates the perfect ecosystem for Cutibacterium acnes to multiply exponentially.
- Inflammation Cascade: C. acnes secretes enzymes that break down sebum into irritating free fatty acids. This action breaches the follicular wall, leaking contents into the dermis and triggering an influx of neutrophils and inflammatory cytokines.
Signs & Symptoms
Acne vulgaris primarily targets areas of the body with the highest density of sebaceous glands: the face, chest, upper back, and shoulders. Beyond the physical presence of spots, symptoms include localized warmth, tenderness, and throbbing pain in severe cases.
Dermatologists classify acne into three distinct severity levels to guide acne treatment:
| Severity Level | Clinical Presentation | Primary Lesion Types |
| Mild | Confined mostly to the face; minimal inflammation. | Primarily open and closed comedones; fewer than 15-20 papules/pustules. |
| Moderate | Visible redness and wider distribution across the face and torso. | A mix of multiple papules, pustules, and occasional nodules. |
| Severe | Widespread, deeply inflamed, painful, and prone to structural tissue damage. | Numerous painful nodules, large cysts, and extensive scarring. |
Diagnosis
In the vast majority of cases, a dermatologist performs a clinical diagnosis based on a physical examination of the skin under proper lighting.
When Further Medical Investigations Are Needed
Diagnostic testing is reserved for patients exhibiting signs of underlying endocrine abnormalities. A hormonal evaluation is warranted if a female patient presents with acne alongside irregular periods, hirsutism (excess face/body hair), or male-pattern hair loss.
Suspicion of Polycystic Ovary Syndrome (PCOS) or adrenal hyperplasia prompts blood tests to evaluate:
- Free and total testosterone
- Dehydroepiandrosterone sulfate (DHEA-S)
- Luteinizing hormone (LH) and follicle-stimulating hormone (FSH)
Complications
Acne is a self-limiting condition for many, but its architectural and psychological structural damage can be permanent.
Physical Complications
- Acne Scars: Permanent structural changes resulting from altered collagen remodeling during the healing process. These include atrophic scars (icepick, rolling, and boxcar scars) and hypertrophic or keloid scars (raised, firm tissue bundles).
- Post-Inflammatory Hyperpigmentation (PIH): Flat, discolored spots left behind after an inflammatory lesion heals. This condition is especially common and long-lasting in darker skin types (Fitzpatrick phototypes IV-VI).
Psychological Impact
Because acne alters facial appearance during formative years, it carries a heavy psychological burden. Studies consistently link acne to heightened rates of clinical anxiety, depression, social withdrawal, and low self-esteem.
Management and Acne Treatment
Effective acne management requires a tailored approach combining daily skincare, targeted medications, and clinical procedures.
A. General Skincare Measures
The foundation of any acne routine relies on preserving the skin barrier:
- Gentle Cleansing: Wash the face no more than twice daily using a mild, soap-free, pH-balanced cleanser. Aggressive scrubbing strips essential lipids, triggering compensatory oil production.
- Non-Comedogenic Products: Ensure all moisturizers, sunscreens, and makeup items are explicitly labeled “non-comedogenic” or “oil-free” to prevent physical pore blockage.
B. Pharmacological Treatment
Medical therapies target specific arms of the pathophysiology matrix.
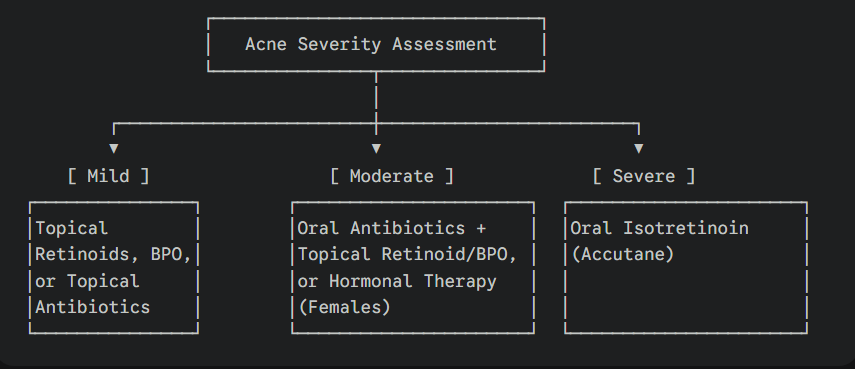
Topical Therapies (Mild to Moderate Acne)
- Benzoyl Peroxide (BPO): An antimicrobial agent that introduces oxygen into the pore, killing C. acnes without generating bacterial resistance. It also helps dissolve keratin plugs.
- Topical Retinoids (Tretinoin, Adapalene, Tazarotene): Vitamin A derivatives that normalize follicular keratinization, preventing comedone formation and accelerating cell turnover.
- Topical Antibiotics (Clindamycin, Erythromycin): Used to reduce bacterial loads and dampen inflammation. They should always be paired with benzoyl peroxide to prevent bacterial mutations.
Oral Therapies (Moderate to Severe Acne)
- Oral Antibiotics (Doxycycline, Minocycline, Azithromycin): Used for short courses (typically under 3-4 months) to calm widespread inflammatory acne.
- Oral Isotretinoin: A highly effective systemic retinoid reserved for severe, scarring, or treatment-resistant nodulocystic acne. It systematically shuts down excess oil production, shrinks sebaceous glands, and normalizes skin shedding.
⚠️ Clinical Note: Oral isotretinoin is highly teratogenic (causes severe birth defects). Female patients of childbearing potential must adhere to strict contraceptive protocols (such as iPLEDGE) while undergoing treatment.
Hormonal Therapy (For Female Patients)
- Oral Contraceptive Pills (OCPs): Specific FDA-approved birth control pills containing estrogen and progestin help suppress ovarian androgen production.
- Spironolactone: An oral anti-androgen block that prevents testosterone from binding to sebaceous receptors, directly reducing sebum output.
C. Procedural Treatments
In-office procedures supplement medical therapies to accelerate clearance and treat acne scars:
- Chemical Peels: Salicylic acid or glycolic acid peels chemically exfoliate the epidermis and clear out follicle linings.
- Laser and Light Therapies: Photodynamic therapy (PDT) and fractionated lasers target C. acnes bacteria or heat sebaceous glands to lower oil production and stimulate collagen for scar repair.
- Comedone Extraction: Mechanically clearing stubborn whiteheads and blackheads using sterile tools to prevent inflammatory rupture.
Prevention
Maintaining clear skin requires sustainable lifestyle adjustments alongside consistent medical treatments:
- Shower Post-Exercise: Wash acne-prone skin immediately after sweating to clear away trapped salts, oils, and bacteria.
- Manage Diet: Reduce high-glycemic snacks and refined sugars. Consider lowering dairy intake if a personal correlation with flare-ups is observed.
- Sanitize Contact Surfaces: Clean items that frequently touch the face, such as cell phone screens and pillowcases, to minimize bacterial transfer.
Red Flag Signs
While acne is rarely a medical emergency, certain clinical signs require urgent dermatological intervention:
- Sudden, Explosive Onset: Rapid development of severe acne paired with systemic symptoms like fever, joint pain, and fatigue (a rare condition known as Acne Fulminans).
- Signs of Virilization: Acne accompanied by rapid voice deepening, male-pattern baldness, or clitomegaly in females, suggesting an androgen-producing tumor.
- Rapid Scarring: Quickly developing deep, structural depressions in the skin requires immediate intervention to prevent lifelong scarring.
Patient Education Tips
Managing expectations is a vital component of successful acne care.
The Do’s and Don’ts Checklist
- DO give new medications at least 6 to 8 weeks to work. Skin remodeling and clearance happen slowly.
- DO apply topical retinoids to the entire affected area, not just as a spot treatment, to treat invisible microcomedones before they surface.
- DON’T pick, squeeze, or pop pimples. Doing so forces inflammatory material deeper into the dermis, multiplying the risk of infection and permanent acne scars.
- DON’T use harsh, grainy physical scrubs, which rupture healing skin cells and worsen inflammation.
Frequently Asked Questions (FAQs)
Does wearing makeup make acne worse?
Not necessarily, provided you select the right formulas. Look for oil-free products specifically labeled “non-comedogenic.” Always remove makeup thoroughly before sleeping using a gentle, non-stripping cleanser.
Why am I getting acne as an adult when I never had it as a teenager?
Adult-onset acne is highly common, particularly in women. It is primarily driven by fluctuating hormone levels associated with stress, menstrual cycles, starting or stopping birth control pills, or underlying conditions like PCOS.
How long does it take for acne treatments to show visible results?
Skin cells take roughly 28 to 30 days to cycle. Consequently, most evidence-based acne treatments require 6 to 12 weeks of consistent daily use before you notice significant, visible clearance.
Can washing my face more often clear up my pimples?
No. Acne is not caused by poor hygiene. Washing your face more than twice a day strips natural lipids, compromises your skin barrier, and triggers irritation, which can actually increase oil production and worsen breakouts.
What is the difference between purging and breaking out?
Purging occurs when active ingredients like retinoids or chemical peels accelerate skin cell turnover, causing preexisting microcomedones to surface all at once. This phase typically lasts 4–6 weeks, and the lesions appear in areas where you normally get acne. A standard breakout represents a negative reaction to a product, resulting in new lesions in entirely new areas that take longer to heal.
Conclusion
Acne vulgaris is a highly dynamic medical condition driven by clear physiological mechanisms, not personal hygiene or lifestyle shortcomings. While it can be a challenging journey physically and emotionally, remember that virtually every case of acne can be successfully controlled with the right combination of medical guidance, patience, and evidence-based care. If over-the-counter options fail to provide relief, consult a board-certified dermatologist to build a customized treatment plan that protects both your skin structure and your peace of mind.
“This content is for informational and educational purposes only and is not intended as medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any medical decisions.”