Introduction
Prescribing, dispensing, and administering medications to pediatric patients requires a high level of clinical accuracy. In adult medicine, standard “one-size-fits-all” dosing protocols are common. For adults, a standard tablet or capsule of an antibiotic, analgesic, or antihypertensive is usually prescribed without calculating the patient’s specific body weight or metabolic capacity. In pediatrics, this approach is dangerous.
To calculate pediatric drug doses safely, healthcare professionals must move away from adult-centric paradigms and treat every child as a unique pharmacokinetic entity. The physiological differences between infants, children, and adults mean that a minor calculation error can lead to therapeutic failure or severe toxicity.
According to epidemiological studies on patient safety, medication errors occur up to three times more frequently in pediatric care environments than in adult settings. The vast majority of these errors stem from calculation mistakes during weight-based dosing.
This comprehensive guide breaks down the science of pediatric pharmacology, explains the math behind weight-based calculations, and provides clinical safety workflows designed to eliminate medication errors.
Understanding Pediatric Drug Doses Safely
To prescribe pediatric drug doses safely, clinicians must understand why children require specialized dosing strategies. The phrase “children are not small adults” is a core principle of pediatric medicine.
From birth through adolescence, a human body undergoes continuous physiological development that affects how drugs are handled. Developmental pharmacology evaluates these dynamic changes and maps them to clinical drug administration.
Developmental Pharmacokinetics (ADME)
[Drug Administration]
│
▼
┌───────────┐ ┌──────────────┐
│Absorption │ ───> │ Distribution │
└───────────┘ └──────────────┘
│
▼
┌──────────────┐ ┌───────────┐
│ Metabolism │ ───> │ Excretion │
└──────────────┘ └───────────┘1. Absorption
Gastrointestinal absorption in pediatric patients changes significantly throughout infancy. Neonates possess a higher gastric pH (often > 4) due to immature gastric acid secretion. This alters the bioavailability of acid-labile drugs (like penicillin, which is absorbed more efficiently) and weak acids (like phenobarbital, which is absorbed less efficiently).
Additionally, prolonged gastric emptying times and unpredictable intestinal motility in infants can delay the time required to reach peak plasma drug concentrations. Skin absorption is also enhanced in infants due to a thinner stratum corneum and a larger surface-area-to-weight ratio, increasing the risk of systemic toxicity from topical medications.
2. Distribution
The composition of the human body changes with age. Neonates and young infants have a higher percentage of total body water (up to 80% in preterm newborns) compared to adults (around 60%). Consequently, water-soluble drugs (such as aminoglycosides) require higher milligram-per-kilogram (mg/kg) initial loading doses in infants to achieve therapeutic serum concentrations.
Conversely, infants have a lower percentage of adipose tissue, which decreases the volume of distribution for lipid-soluble drugs. Plasma protein binding is also reduced in newborns because of lower circulating concentrations of albumin and alpha-1-acid glycoprotein. This leads to higher circulating fractions of free, pharmacologically active drug, increasing both therapeutic effects and toxicity risks.
3. Metabolism
The liver is the primary organ responsible for drug biotransformation. Hepatic enzyme systems, specifically the cytochrome P450 (CYP) isoenzymes, mature at different rates. For instance, CYP3A4 and CYP2D6 activity is low at birth but accelerates during early childhood, sometimes exceeding adult metabolic rates on a per-kilogram basis by toddlerhood.
Phase II conjugation pathways, such as glucuronidation, are significantly immature in neonates. A historic example of this is Gray Baby Syndrome, which occurs when neonates cannot metabolize chloramphenicol because of an immature UDP-glucuronosyltransferase enzyme system.
4. Excretion
Renal drug elimination depends on glomerular filtration, tubular secretion, and tubular reabsorption. The glomerular filtration rate (GFR) is low at birth, particularly in preterm infants, and increases over the first few weeks of life, reaching adult levels by approximately 8 to 12 months of age.
Medications cleared primarily by the kidneys (such as ampicillin, gentamicin, and vancomycin) require prolonged dosing intervals or adjusted doses in neonates to prevent accumulation and subsequent toxicity.
For an in-depth review of pediatric drug development, review our comprehensive Pediatric Pharmacology Guide.
Why Weight-Based Dosing Is Used in Pediatrics
Because a child’s body composition, organ size, and metabolic capacity change as they grow, fixed adult doses cannot be safely applied. Instead, pediatric medicine relies primarily on weight-based dosing (mg/kg) or body surface area (BSA) dosing ().
Weight-based dosing scales the amount of active drug to the total mass of the patient. This helps maintain stable drug concentrations across different age groups.
Clinical Rationale for Weight-Based Scaling
- Organ-to-Mass Proportions: Although a toddler weighs a fraction of an adult, their liver and kidney weights relative to total body mass are higher. Weight-based dosing accounts for these scaling factors more accurately than age-based rules (such as Clark’s Rule or Young’s Rule), which are now obsolete.
- Narrow Therapeutic Indexes: Many pediatric medications (e.g., digoxin, phenytoin, aminoglycosides) have a narrow margin between therapeutic success and toxic danger. Dosing by body weight helps keep serum levels within safe therapeutic ranges.
- Linear vs. Non-linear Parameters: While total clearance of some drugs does not scale linearly with weight, dosing remains the most practical, validated, and accessible method for bedside clinicians to calculate safe pediatric drug doses.
Weight-Based Dosing vs. Body Surface Area (BSA) Dosing
While weight-based dosing is standard for general pediatric medicines, BSA dosing () is preferred for medications that require higher precision, such as chemotherapeutic agents, certain antiretrovirals, and specific critical care medications.
BSA correlates with cardiac output and renal blood flow. However, because measuring height and calculating BSA can be complex in emergency settings, body weight in kilograms remains the standard metric for daily pediatric drug dosing.
Basic Principles of Pediatric Dose Calculation
Before calculating pediatric drug doses, clinicians must understand the terminology used in pediatric prescriptions.
Key Concepts
Milligrams per Kilogram ()
This indicates the amount of drug to be administered per single kilogram of the child’s body weight. For example, a prescription might read: “Give per dose.”
Milligrams per Kilogram per Day ()
This specifies the total cumulative amount of drug the patient should receive over a 24-hour period. This total dose is often split into multiple smaller doses throughout the day.
Divided Doses
This tells the clinician to split the calculated total daily dose into equal portions. For instance, if a daily dose is divided every 12 hours, the patient receives at each administration.
Maximum Daily Dose (Dose Capping)
Pediatric weight-based doses should never exceed the maximum recommended adult dose for the same indication. Once a child’s weight-based dose equals or exceeds the adult dose, the dose must be capped at the adult limit.
Age-Specific Restrictions
Certain drugs are contraindicated or require unique dosing regimens within specific age brackets, regardless of weight, due to developmental toxicity risks (e.g., ceftriaxone in neonates due to hyperbilirubinemia risks).
Common Units Used in Pediatric Dosing
Accurate calculations depend on consistent unit measurement. Mixing up units—such as confusing milligrams () with milliliters () or micrograms () with milligrams ()—is a frequent cause of pediatric medication errors.
Core Units
- Milligram (): The mass of the active drug ingredient.
- Microgram ( or ): Used for highly potent medications. Always write out “mcg” to prevent confusion with “mg”.
- Gram (): Used for large-mass medications like certain bulk laxatives or IV immunoglobulins.
- Kilogram (): The standard unit for patient weight. Pounds () must always be converted to kilograms.
- Milliliter (): The volume of liquid medication that contains the dissolved drug.
Dosing Conversion Reference Table
The table below outlines the standard metric conversions required for precise pediatric calculations.
| To Convert From | To | Multiplier / Operation | Clinical Example |
| Pounds () | Kilograms () | Divide by | A child weighs () |
| Kilograms () | Pounds () | Multiply by | A child weighs () |
| Grams () | Milligrams () | Multiply by | of ceftriaxone = |
| Milligrams () | Micrograms () | Multiply by 1,000 | of digoxin = |
| Micrograms () | Milligrams () | Divide by 1,000 | of fentanyl = |
Formula for Weight-Based Dosing
To calculate pediatric drug doses accurately, you need to master three fundamental formulas.
Formula 1: Calculating the Individual Target Dose
This formula determines the total milligrams needed for a single dose based on a single-dose recommendation.
Dose\ (mg) = Patient\ Weight\ (kg) \times Recommended\ Dose\ (mg/kg)
Formula 2: Calculating Total Daily Dose
This formula calculates the total amount of medication required over a full 24-hour period.
Total\ Daily\ Dose\ (mg/day) = Patient\ Weight\ (kg) \times Recommended\ Daily\ Dose\ (mg/kg/day)
Formula 3: Calculating the Single Split Dose
When a daily dose needs to be spread out across multiple administrations, use this formula to find the size of each individual dose.
Individual\ Dose\ (mg) = \frac{Total\ Daily\ Dose\ (mg/day)}{Number\ of\ Doses\ Per\ Day}Worked Math Examples
Example A: Single Dose Calculation
A clinician wants to administer single-dose paracetamol to a child weighing . The target recommendation is .
Dose = 12\ kg \times 15\ mg/kg = 180\ mg
Example B: Total Daily Dose with Divided Schedule
A pediatric resident prescribes amoxicillin at divided into two daily doses for a child weighing .
- Calculate total daily dose:
- Calculate individual split dose:
Step-by-Step Guide to Calculate Pediatric Drug Doses Safely
To systematically eliminate errors, clinicians should follow this step-by-step clinical calculation workflow before administering any medication.
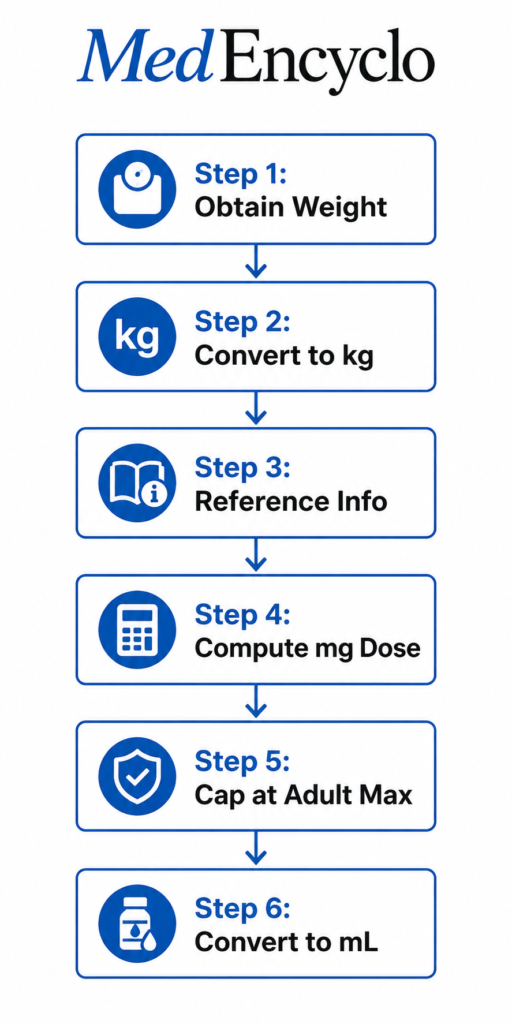
Step 1: Verify the Patient’s Actual Current Weight
Never rely on historical weight records or verbal approximations from family members. Weigh the child directly on a calibrated digital scale at the time of admission or evaluation.
Step 2: Ensure Weight is Recorded in Kilograms
If the scale reads in pounds, convert the value to kilograms immediately using the standard conversion factor (). Double-check this step, as entering a pound value as kilograms will result in an overdose of more than double the intended amount.
Step 3: Consult Reliable Prescribing Reference Materials
Check authoritative pediatric guidelines like the British National Formulary for Children (BNFc) or the Harriet Lane Handbook to verify the correct range for the specific clinical indication.
Step 4: Calculate the Required Dose in Milligrams
Apply the standard formula:
\text{Weight (kg)} \times \text{Dosing Parameter (mg/kg)}Step 5: Check Against the Maximum Adult Dose
Compare the calculated milligram value with the standard adult dose for the same condition. If the calculated pediatric dose is higher than the adult dose, cap it at the adult maximum.
Step 6: Convert the Milligram Dose into Volumetric Milliliters ()
For liquid oral medications or intravenous solutions, calculate the volume to draw up based on the product’s concentration:
Volume\ (mL) = \frac{Desired\ Dose\ (mg)}{Liquid\ Concentration\ (mg/mL)}Step 7: Perform an Independent Double-Check
Before preparing or giving the drug, have a colleague independently run the calculations from scratch to confirm the final volume.
Clinical Pearl: When converting milligrams to milliliters, always verify the bottle’s label. Liquid medications often come in multiple concentrations (for example, amoxicillin is available as . Using the wrong concentration configuration can lead to major dosing errors.
For more information on reducing risks during drug administration, check out our guide on Medication Error Prevention.
Pediatric Drug Doses Safely for Common Medications
This section outlines standard clinical dosing parameters and worked math examples for seven common pediatric medications.
1. Paracetamol (Acetaminophen)
- Standard Pediatric Reference Dose: every 4 to 6 hours as needed. Maximum daily limit: (up to ).
- Clinical Scenario: A 14-month-old child presenting with a fever weighs . The available suspension is calibrated at .
- Step-by-Step Calculation:
- Target dosage chosen:
- Compute required weight-based milligrams:
- Determine the stock solution concentration:
- Calculate the liquid dose volume:
- Safety Considerations: Accidental paracetamol overdoses are a leading cause of acute liver failure in children. Always confirm the concentration on the packaging, as infant drops () vary by region.
2. Ibuprofen
- Standard Pediatric Reference Dose: every 6 to 8 hours. Maximum daily limit: .
- Clinical Scenario: A 6-year-old child presenting with acute otitis media pain weighs . The available stock concentration is .
- Step-by-Step Calculation:
- Target dosage chosen:
- Compute required weight-based milligrams:
- Determine the stock solution concentration:
- Calculate the liquid dose volume:
- Safety Considerations: Ensure the child is well-hydrated before administration. Ibuprofen should be avoided in infants under 6 months of age due to immature renal function and clearance mechanics.
3. Amoxicillin
- Standard Pediatric Reference Dose:
- Mild-to-moderate infections: split into two or three doses.
- High-dose strategy for Acute Otitis Media: split into two doses every 12 hours.
- Clinical Scenario: An 18-month-old infant diagnosed with acute otitis media weighs . The stock amoxicillin suspension concentration is .
- Step-by-Step Calculation:
- Target high-dose regimen:
- Compute total milligrams for a 24-hour period:
- Split into two equal doses (every 12 hours):
- Determine the stock liquid concentration factor:
- Calculate the liquid volume needed for each dose:
- Safety Considerations: High-dose amoxicillin can cause gastrointestinal side effects, including diarrhea. Ensure parents use a precise oral syringe rather than a standard kitchen spoon to measure the dose.
4. Cefixime
- Standard Pediatric Reference Dose: administered as a single daily dose or split into two equal doses every 12 hours.
- Clinical Scenario: A 4-year-old child with a urinary tract infection weighs . The available oral suspension concentration is .
- Step-by-Step Calculation:
- Target dosage chosen: as a single dose.
- Compute required weight-based milligrams:
- Determine the stock solution concentration:
- Calculate the liquid dose volume:
- Safety Considerations: Adjust the dose if the patient has known renal impairment. Shake the suspension thoroughly before measuring to ensure the drug is evenly distributed.
5. Azithromycin
- Standard Pediatric Reference Dose: on day 1, followed by as a single dose on days 2 through 5.
- Clinical Scenario: A 5-year-old child diagnosed with atypical community-acquired pneumonia weighs . The available suspension concentration is .
- Step-by-Step Calculation:
- Day 1 (Loading Dose):
- Target dosage:
- Compute weight-based milligrams:
- Stock concentration:
- Calculate volume:
- Days 2–5 (Maintenance Dose):
- Target dosage:
- Compute weight-based milligrams:
- Calculate volume:
- Day 1 (Loading Dose):
- Safety Considerations: Azithromycin can cause QT-interval prolongation. Review the patient’s medication history for any interacting drugs.
6. Salbutamol (Albuterol Syrup)
- Standard Pediatric Reference Dose: Oral syrup route: administered three to four times daily.
- Clinical Scenario: A 3-year-old child with reactive airway disease weighs . The available syrup concentration is .
- Step-by-Step Calculation:
- Target dosage chosen:
- Compute required weight-based milligrams:
- Determine the stock solution concentration:
- Calculate the liquid dose volume:
- Safety Considerations: Inhaled delivery via a metered-dose inhaler (MDI) with a spacer is preferred over oral syrups due to fewer systemic side effects. Monitor the patient for tachycardia, tremors, and hypokalemia if oral syrups are used.
7. Ondansetron
- Standard Pediatric Reference Dose: intravenously or orally every 8 hours as needed for gastroenteritis-induced vomiting.
- Clinical Scenario: A 7-year-old child presenting with dehydration and persistent vomiting weighs . The available oral disintegrating solution or soluble formulation is .
- Step-by-Step Calculation:
- Target dosage chosen:
- Compute required weight-based milligrams:
- Determine the stock solution concentration:
- Calculate the liquid dose volume:
- Safety Considerations: Do not exceed a single dose of in pediatric patients. Ondansetron can prolong the QT interval; use caution in patients with underlying cardiac conditions.
Pediatric Drug Doses Safely in Infants
Calculating drug doses for infants requires extra caution. This group is divided into specific developmental stages:
- Preterm Infants: Born before 37 weeks of gestation.
- Neonates: From birth up to 28 days of life.
- Infants: From 28 days up to 1 year of age.
During these early stages of life, organ systems change rapidly. A newborn’s liver and kidneys can take weeks to develop full metabolic and excretory capacity.
Key Precautions for Infant Dosing
Extended Intervals
Because neonates have a lower glomerular filtration rate, drugs like gentamicin or ampicillin require extended dosing intervals (e.g., every 12, 18, or 24 hours) compared to older infants (every 6 to 8 hours).
Avoid Certain Excipients
Infant formulations must be free from harmful additives. Preservatives like benzyl alcohol can cause fatal systemic toxicities (“gasping syndrome”) in neonates. Propylene glycol, often found in liquid preparations, can also accumulate and lead to central nervous system depression.
TDM (Therapeutic Drug Monitoring)
For high-risk medications, rely on plasma serum concentrations rather than weight-based calculations alone. Adjust maintenance doses based on actual drug levels in the blood.
Pediatric Drug Doses Safely in Obese Children
The rising prevalence of childhood obesity introduces additional complexity to weight-based calculations.
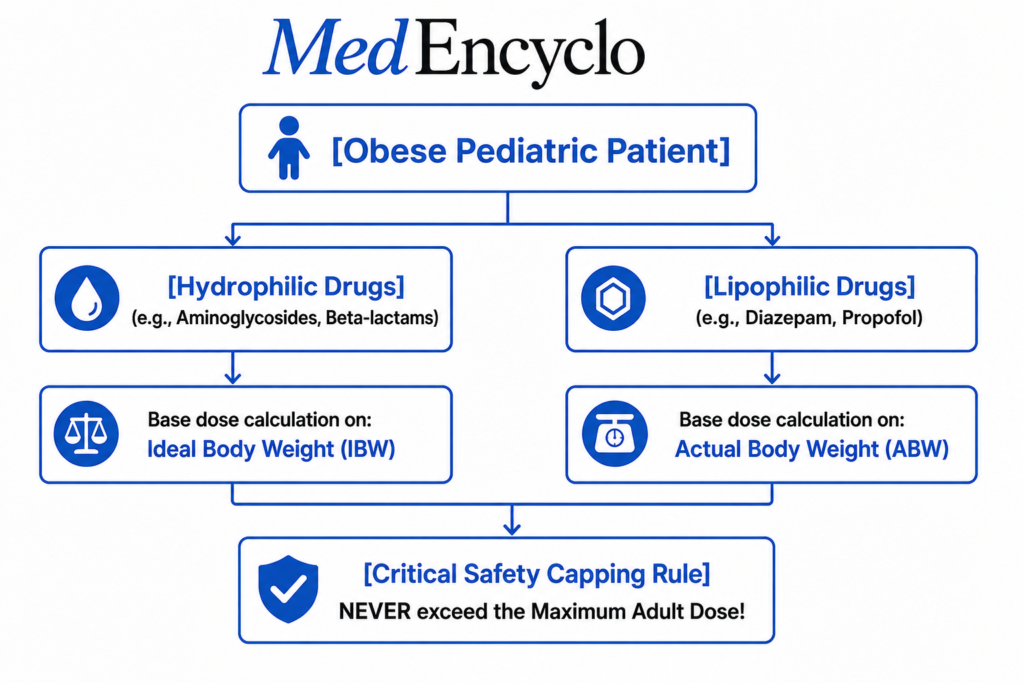
If a clinician uses actual body weight () to calculate hydrophilic drug doses for an obese child, the serum concentration can reach toxic levels. This occurs because hydrophilic medications do not distribute into excess adipose tissue.
Weight Definitions for Dosing
Actual Body Weight ()
The patient’s true weight measured on a scale.
Ideal Body Weight ()
The standard weight expected for a child of a specific height, sex, and age, determined using growth charts from organizations like the Centers for Disease Control and Prevention (CDC).
Adjusted Body Weight ()
A calculated weight value used for specific medications with a narrow therapeutic index. It bridges the gap between ideal and actual weight:
AdjBW = IBW + [0.4 \times (ABW - IBW)]
Clinical Rules for Obese Pediatric Dosing
- For Hydrophilic Medications (e.g., Aminoglycosides, Methylprednisolone): Base the initial weight-based calculation on the child’s Ideal Body Weight () to prevent overdosing.
- For Lipophilic Medications (e.g., Diazepam, Valproate): Base the calculations on Actual Body Weight (), as these drugs distribute widely into fat tissues.
- The Overriding Rule: Regardless of the weight metric used, never exceed the maximum adult dose for the medication.
Importance of Maximum Dose Limits (Dosing Caps)
A common mistake in pediatric medicine is continuing to scale doses linearly as a child’s weight increases, without checking adult limits. This can cause older or heavier children to receive doses significantly higher than the standard adult recommendation.
The Danger of Linear Scaling
Consider a 13-year-old adolescent who weighs . A clinician prescribes amoxicillin for a standard skin infection at a dose of divided every 8 hours.
- Linear Calculation:
- Divided Dose Size:
The standard adult dose for this indication is typically every 8 hours (). Running the calculation linearly exposes the adolescent to an unnecessary overdose. The pediatric dose should have been capped at the adult maximum of per dose.
High-Risk Medications That Require Strict Dosing Caps
- Central Nervous System Stimulants (e.g., Methylphenidate): Must be capped to prevent cardiovascular side effects.
- First-Generation Antihistamines (e.g., Diphenhydramine): Must be capped to avoid dangerous sedation or paradoxical excitation.
- Corticosteroids (e.g., Prednisolone): Must be capped to reduce the risk of acute adrenal suppression.
Common Pediatric Medication Errors and How to Prevent Them
1. Decimal Point Mistakes (The Ten-Fold Error)
Misplacing a decimal point can cause a catastrophic 10-fold or 100-fold error. Writing “” can easily be misread as “” if the decimal point is missed. Conversely, writing “.5 mg” instead of “0.5 mg” can lead to an overdose if the period is overlooked.
- Prevention Strategy: Never use trailing zeros for whole numbers (write ). Always use a leading zero before a decimal point (write ).
2. Confusing Weight Units ()
Entering a child’s weight in pounds into a formula that requires kilograms results in an underdose of approximately . Conversely, entering a kilogram weight into a formula meant for pounds can cause a dangerous overdose.
- Prevention Strategy: Configure electronic prescribing systems to accept patient weights exclusively in kilograms.
3. Concentration Mix-Ups
Assuming all liquid concentrations of a drug are identical is a frequent source of error. For example, liquid paracetamol is available in concentrations of , and high-concentration infant drops.
- Prevention Strategy: Always check the drug label directly and verify the exact concentration () before running your volumetric calculations.
4. Inappropriate Delivery Devices
Using standard kitchen spoons to measure liquid medications introduces significant variance, as their volumes range from .
- Prevention Strategy: Provide clear instructions to parents to use only calibrated oral dosing syringes or graduated medicine cups.
Medication Safety Checklist for Healthcare Professionals
To ensure safety at each stage of the pediatric dosing process, clinicians can follow this structured checklist:
- Verify Weight Accuracy: Is the patient’s weight current, measured within the last 24 hours, and recorded clearly in kilograms?
- Confirm the Clinical Indication: Are you using the correct dosing range for the patient’s specific diagnosis?
- Perform Calculations Independently: Have you run the and volumetric formulas without looking at previous notes?
- Apply Adult Dose Caps: Does the calculated dose stay below the standard maximum adult limit?
- Check the Product Concentration: Have you verified the exact value printed on the stock medication vial or bottle?
- Complete a Secondary Review: Has a qualified colleague independently verified the patient’s weight, calculations, and final prepared volume?
- Select the Right Measuring Tool: Is an appropriately sized oral syringe or clear volumetric device prepared for administration?
To find out more about counseling families on these steps, read our Pediatric Medication Administration guide.
Medication Safety Tips for Parents and Caregivers
When a child is discharged with a prescription, parents become responsible for administering the medication safely. Healthcare professionals should guide them through these essential rules.
Clear Labeling
Make sure parents understand the difference between the drug mass () and the liquid volume (). The prescription label should clearly state the dose in milliliters ().
Use the Right Measuring Tool
Advise parents never to use household kitchen spoons. Provide a calibrated oral syringe or a dedicated medicine cup with the medication.
Double-Check the Strengths
Remind parents to verify the concentration on the box if they switch between different brands or purchase a refill, as liquid concentrations can vary.
Prevent Multi-Medication Overlaps
Educate parents to check ingredient lists on over-the-counter medicines. For example, many cold remedies contain paracetamol; using them alongside standard paracetamol suspension can lead to an accidental overdose.
Special Situations Requiring Extra Caution
Renal Impairment
Children with congenital renal anomalies or acute kidney injury (AKI) cannot clear medications effectively. For drugs like vancomycin, aminoglycosides, or low-molecular-weight heparins, clinicians must extend the dosing interval or reduce the dose based on calculated creatinine clearance ().
In pediatrics, the Modified Schwartz Equation is used to estimate GFR:
eGFR\ (mL/min/1.73m^2) = \frac{k \times Height\ (cm)}{Serum\ Creatinine\ (mg/dL)}(Where is a constant based on the patient’s age and muscle mass development).
Hepatic Impairment
Severe hepatic dysfunction alters drug clearance and protein binding. For medications metabolized by the liver (such as valproic acid, metronidazole, or clindamycin), monitor the child closely for signs of toxicity and adjust doses downward as needed.
Critical Care and Neonatal Intensive Care (NICU/PICU)
Critically ill children often experience rapid fluid shifts, capillary leak syndrome, or altered organ perfusion. Patients undergoing Extracorporeal Membrane Oxygenation (ECMO) or continuous renal replacement therapy (CRRT) require dynamic dosing adjustments managed by a clinical pharmacist, guided by real-time serum drug levels.
Pediatric Drug Doses Safely: Clinical Case Studies
These case studies illustrate how weight-based dosing rules are applied in real-world clinical situations.
Case Study 1: High-Dose Amoxicillin for Acute Otitis Media
- Patient Profile: 11-month-old female with a severe bulging tympanic membrane.
- Recorded Weight:
- Prescription Order: Amoxicillin suspension at divided into two daily doses.
- Stock Drug Concentration Available:
- Clinical Calculation Steps:
- Total daily target milligram dose:
- Divide into individual doses (every 12 hours):
- Determine concentration per milliliter:
- Compute required liquid volume per dose:
- Safety Review: The dose does not exceed the adult limit. Rounding the volume slightly to per dose is clinically acceptable to make measurement practical for the parents.
- Final Recommendation: Administer amoxicillin suspension orally every 12 hours for 10 days.
Case Study 2: Intravenous Gentamicin in a Neonate
- Patient Profile: 3-day-old newborn male suspected of having neonatal sepsis.
- Recorded Weight:
- Prescription Order: Gentamicin IV at every 36 hours (extended interval due to immature neonatal renal clearance).
- Stock Drug Concentration Available: vial.
- Clinical Calculation Steps:
- Compute target milligram dose:
- Compute required liquid volume to draw up from the vial:
- Safety Review: Neonatal clearance is low. Ensure the extended 36-hour interval is programmed correctly into the electronic medical record system to prevent drug accumulation.
- Final Recommendation: Administer of gentamicin intravenously every 36 hours. Order trough serum levels before the third dose.
Case Study 3: Overdose Check for an Obese Adolescent
- Patient Profile: 12-year-old male presenting with acute pharyngitis.
- Recorded Weight: (Actual Body Weight)
- Prescription Order: Azithromycin suspension at orally as a single loading dose on day 1.
- Stock Drug Concentration Available:
- Clinical Calculation Steps:
- Compute weight-based milligrams using actual weight:
- Verify against maximum adult limits: The standard adult loading dose for azithromycin is as a single dose.
- Apply the capping rule: The calculated pediatric dose () is higher than the adult dose (). Cap the dose at .
- Compute liquid volume based on the capped dose:
- Safety Review: Capping the dose avoids systemic gastrointestinal toxicity and potential cardiac side effects like QT prolongation.
- Final Recommendation: Administer a capped dose of orally on Day 1, followed by once daily on Days 2 through 5.
Case Study 4: Liquid Ibuprofen for a Toddler
- Patient Profile: 3-year-old female with a high fever.
- Recorded Weight:
- Prescription Order: Ibuprofen suspension at every 6 hours as needed.
- Stock Drug Concentration Available:
- Clinical Calculation Steps:
- Compute target milligram dose:
- Determine concentration per milliliter:
- Compute required liquid volume per dose:
- Safety Review: The calculated dose falls within the safe therapeutic range. Ensure the family is supplied with a clear oral syringe to measure exactly .
- Final Recommendation: Administer orally every 6 hours as needed for fever.
Case Study 5: Intravenous Ondansetron for Gastroenteritis
- Patient Profile: 5-year-old male with persistent vomiting and mild dehydration.
- Recorded Weight:
- Prescription Order: Ondansetron IV at before initiating oral rehydration therapy.
- Stock Drug Concentration Available: injection vial.
- Clinical Calculation Steps:
- Compute target milligram dose:
- Compute required liquid volume to draw up from the vial:
- Safety Review: The dose stays below the single pediatric ceiling limit of . Administer via slow intravenous injection over 2 to 5 minutes.
- Final Recommendation: Administer of intravenous ondansetron as a single slow push injection.
The Role of Pharmacists in Pediatric Dose Verification
Pediatric clinical pharmacists serve as a critical safety barrier in the medication use process. They review prescriptions to catch errors before drugs reach the patient.
Key Pharmacist Interventions
- Order Review and Verification: Every pediatric medication order undergoes verification against the patient’s current weight, age, and renal function.
- Mismatched Concentration Alerting: Pharmacists ensure the concentration prepared by the pharmacy matches what is configured in the hospital’s smart infusion pumps.
- Medication Reconciliation: Pharmacists cross-reference home medication schedules with inpatient orders to prevent therapeutic duplication or missed doses.
- Clear Parent Counseling: Pharmacists provide clear, practical guidance to families at discharge, demonstrating how to use oral syringes to measure liquid volumes accurately.
Digital Tools and Pediatric Dose Calculators
Computerized Physician Order Entry (CPOE) systems and electronic clinical decision support tools have streamlined pediatric prescribing. These applications automatically calculate weight-based doses based on the patient’s electronic health record.
Benefits and Risks of Automated Systems
While digital calculators help reduce math errors, clinicians must remain vigilant. Entering an incorrect patient weight into a computer system will cause every automated calculation to be wrong.
Similarly, alert fatigue can cause clinicians to overlook critical system warnings regarding maximum dose overrides.
Digital tools should always be treated as secondary aids. They do not replace the need for manual mathematical verification by qualified healthcare professionals.
Reputable Professional References
- The Harriet Lane Handbook (Johns Hopkins Medicine)
- British National Formulary for Children (BNFc)
- Lexicomp Pediatric & Neonatal Dosage Handbook
- Micromedex NeoFax Essentials
Frequently Asked Questions (FAQ)
Why is pediatric dosing based on weight instead of age?
Age does not accurately reflect a child’s physiological development or metabolic capacity. Two 4-year-old children can vary significantly in body mass and composition. Basing doses on weight ensures the amount of active drug matches the child’s actual body mass, which helps maintain safe and effective concentrations in the blood.
How often should a child’s weight be updated for dosing calculations?
In inpatient hospital environments, children should be weighed daily to account for rapid growth or fluid shifts. In outpatient clinics, weight must be re-measured at every visit before prescribing a new medication. Never rely on historical records or parent approximations.
Can I use standard adult doses for older children?
Only if the calculated weight-based pediatric dose meets or exceeds the standard adult dose. Once a child’s weight-based calculation equals the adult dose, the dose must be capped at the adult maximum. Never exceed the adult limit, as doing so can lead to dangerous systemic toxicity.
Why are some liquid medications available in multiple concentrations?
Manufacturers produce varying concentrations to accommodate different age brackets. Infants require highly concentrated drops so they can receive their necessary dose in a very small volume of liquid. Older children need larger, less concentrated volumes to allow for precise measurement as their dosage requirements increase.
What are the signs that a child has received a medication overdose?
Symptoms depend on the specific class of medication. Common signs of toxicity include extreme lethargy, slow or shallow breathing, persistent vomiting, unexplained skin rashes, tachycardia, or sudden changes in behavior. If an overdose is suspected, seek immediate emergency medical care or contact emergency poison control services.
Conclusion
Calculating pediatric drug doses safely requires clinical precision, an understanding of developmental pharmacology, and adherence to strict verification workflows. Because children experience rapid changes in body mass and organ function as they grow, fixed adult dosing models cannot be safely applied.
By systematically following weight-based calculation steps, double-checking liquid concentrations, applying adult dose caps, and performing independent secondary reviews, healthcare professionals can significantly reduce medication errors.
Whether you are working in an emergency department, a neonatal intensive care unit, or a community pharmacy, maintaining a rigorous approach to calculation safety is essential for protecting young patients and delivering safe, effective care.
External References
- World Health Organization (WHO): Pocket Book of Hospital Care for Children
- American Academy of Pediatrics (AAP): Policy Statement on Pediatric Medication Safety
- Food and Drug Administration (FDA): Guidance on Pediatric Dosing and Labeling Regulations
- British National Formulary for Children (BNFc): Official Pediatric Dosage Guidance Compendium
“This content is for informational and educational purposes only and is not intended as medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any medical decisions.”




